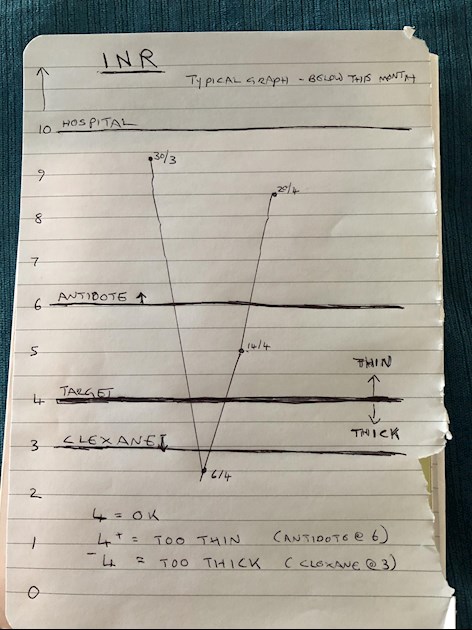
This constant swinging is ruining my life. It makes me so ill. Getting very down and depressed. My diet is as advised. I’m Lupus anticoagulant positive. Here is a graph of this months readings, last 4 tests.
It has been suggested that maybe I don’t metabolise vit K properly. Anyone had that problem? I’m going to be tested once COVID is over. (Does anyone know how?)
I always crash drastically when given the antidote (vit k) even just 2mls.
Written by
WendyWoo50
To view profiles and participate in discussions please or .
I wonder if it’s possible you might be a poor metabolized of warfarin.
Vkorc1.
I have one copy, so I can still take warfarin. I just need a bit more, that’s all .
I take between 18.25 and 20 mg each evening.
It doesn’t matter how much I take- and yes I am Triple positive also- but not always positive for LA, it comes and goes. ( I think it’s why my graph can bounce.)
My target in between 5.0 and 5.5
If it goes to 6 I don’t worry. If it goes to 6.25 I just sauté extra spinach.
I do get blood draws three times a week and I manage my greens as if they are medicine.
I’m very steady with my greens, and bump things a little bit up or down Accor to INR results, Greens up or down work in 12-15 hours - tells me what to do with my warfarin- it’s a fine tunes orchestra- the interplay with greens and warfarin. And then I bump up with the clexane if I fall to 4.8 . ( a small amount only.)
If it’s 4.5 then it’s a larger dose of clexane.
This is what I have worked out with my Hematologist.
I’m not so sure if it’s a vitamin k issue your having an issue metabolizing, or the warfarin. (
looks a bit like mine on Warfarin! Could never keep a constant INR. Is this new for you with Warfarin? Or have you always had this problem? I have Clexane twice a day + 100mg Aspirin-so far so good even though I clotted with Clexane previously but (I think) I wasn't also on Aspirin at that time.
I was going to trial clexane twice daily but even after a couple of injections my stomach turns black and each injection has an egg sized lump under it. It lasts for weeks.
I was thinking of buying a self tester but as they can’t be relied upon over 6 When a vein test is required - it wouldn’t be very useful after all.
I hope you can check in with your main consultant by phone or email, for a bit of fine tuning and reassurance. I have never taken Warfarin, so don't have that personal knowledge myself. MaryF
I have never had such dramatic swings. I am sorry to see yours continue. I can only suggest keeping a meticulous log of food and activities and then, seeing if you note a pattern.
Wendy, I can drop to 3.5, then in a week or two be up to 9.
In feb I went to the hospital with a horrific migraine because I was at 8.8 in the afternoon-and needed to rule out a brain bleed. It was clean- no bleed.
A high INR must be checked out to make sure of no bleed. ( especially with a very unusually bad migraine- which I had.)
The time line was this: I was drawn 12:30 in the afternoon and the INR Result was right at 8.8
I sautéed a big dose of fresh spinach. Maybe 1 cup uncooked. I tied in with my doctor and let him know what I was doing.
The migraine got worse. By 10:00pm I went to the hospital to gave the scan. It was clear. Also, my INR was redrawn and it was 5.59
Spinach right away can make a big difference. Get a little bit of chicken broth in a sautés pan and salt ( very slightly saltier than to normal taste) it and bring to a simmer. Then add the fresh spinach. The salt goes in the spinach and will not let the Vitamin k or nutrients out- ( osmotic membrane) the salt will lock in.
Unless you have had a registered dietitian advise you otherwise. ( kidney issues might require you to use very restricted salt amounts, for example.)
You can also do this with fresh frozen spinach as well.
I had trouble with that migraine for three weeks after...February was a particularly rough month for me.
I had a hematologist tell me the body does not like rapidly shifting INR’s
That’s right! It’s such an important issue- trying to self advocate, yet at the same time stay compliant to both our bodies, our hard working physicians, and criteria that usually works- but doesn’t for Some ( most?) APS patients.
I’m starting to wonder if Wendy might need her target moved to 4.5 ish.
Perhaps it’s time to ask her APS specialists hematologist that question.
Understandable warfarin made me crazy but fortunately i am able to tolerate the lovenox/enoxaparin every twelve hours daily. Dont be ashamed-we understand and feel bad for you🥴
No, not at all- don’t ever apologize! How can you know if your symptoms are ,”normal” if you don’t ask?
You do swing more often than I do.
Also- I’m wondering ( and I really hesitate to put this on here... ) do you really need an antidote at 6.0? 6.0 is not safe for you- I understand this.
But It this causing your swings? Another APS patient on here was told by her specialty APS hematologist that the reversal will destabilize the INSr for up to 6 weeks because it’s chemical, and not natural, IF ( that’s a big of) I understood her correctly.
I wish you could be tested ( by vein- I believe you are not a candidate for the finger prick method- I am not as I run my INT too high) more frequently. Tuesday and Friday would be ideal- and an outside ( out of doors) facility.
I know some GP surgeries are setting them up in the UK currently. Or can a phlebotomist come to your home? To the front door area? Front Garger? Side Garden?
Additionally-
I mentioned once before:
Fondaparinux is Once daily injection of synthetic clexane.
Prof Bev Hunt recommends it for some APS patients who fit a specific profile. My London lupus center specialist told me about this in early December.
Usually it’s reserved for:
1. Patients who have refractory APS - keep clotting through Warfarin and clexane- or have problems with clexane
2. It’s especially beneficial for some reason in neurological issues in APS.
It doesn’t tend to sting,
As you know- there will be a give a take. It might be worth a discussion with your hematologist.
Ok, it doesn’t look like warfarin is a good medication for you. It also looks as though they are making things worse by giving you the antidote. Or they are dropping your dosage too far after you have gone so high. Can they try just missing a warfarin dose instead of giving you antidote? You are going into a kind of yo-yo mode with what they are doing now. Could they try smaller changes in your dosages? Do they know about APS and the fact that we can be very sensitive to changes of dose?
If this is the best they can do but they want to keep you on a vitamin K antagonist then could they try you on sinthrome (acenocoumarol) to see if you would stabilise on that instead. It works in a similar way to warfarin.
I know someone that Prof Hunt has put on fondaparinux as she couldn’t take warfarin and she is finding it better. So I agree with Kelly that this might be something for them to consider. But it needs a really knowledgeable consultant to decide that.
I would like to see your dosages on the graph as that might help to see what they are doing.
In the twenty plus years I’ve been on warfarin I’ve never had a stable INR goes up and down as it pleases.
Personally I would never take VitK with an INR of six, it stays in your system too long. But do remember this is only my personal opinion and we are all different.
I’ve had plenty of clots over the years and despite having some ridiculous high INRs up in the high teens have not had a bleed.
The only time I have had a ‘bleed’ was earlier this year and not convinced it was due to Warfarin INR was about 10.8.
I have dodgy lungs and was on loads of meds and started coughing up some not nice stuff.
Even then the docs didn’t think VitK was advisable and within a couple of days was back to where it should be.
Do remember we are all different and what’s good for one is not always good for another.
I can’t add to the good advice here, but just tell you my experience. In the 10 1/2 years I was on warfarin (brand Jantoven) I was never stable. I was always at odds with the coag clinic, who didn’t like what my hematologist said. She was okay when my INR was 6+ and didn’t want me to skip a dose. I watched my Vit K intake religiously, aiming for 120 mcg per day from varying sources of food. I also took 100 mcg of Vit K per day in a tablet, my hemo hoped this addition might stabilize my INR, but it made no difference. I had frequent blood draws and was always black and blue from it.
I’m triple positive, LA, sjogrens and hashimotos. I had no test on the warfarin, none was ever suggested, but I am doing much better on apixiban (over 2 yrs now. I was changed due to extreme migraines). I also take an aspirin daily.
I hope they will find a way to test you so you what is going on.
I’m going to take a small liberty here , and add a few details Preemptively for safety sake and to answer a few questions that might come up:
1. Tofino 5 made this switch to Apixiban under the care of an world renown APS specialist Rheumatoligist who works in tandem with a hematologist. This Rheumatoligist doses Apixiban a bit higher for a APS patients than for non APS patients.
( also even within this physician’s own APS patient population, she might dose one patients slightly higher over another, depending upon clotting history- in otherwords- similarity to how you would set an INR. )
2. This physician keeps extremely close tabs on patient, and if any change occurs, the dose can be changed within 12 hours, ( up or down depending on APS symptoms) or medication changed if necessary.
3. The vast majority of this physicians APS patients do well on this medication protocol. Yes, it’s a small sample size, but that said, there is not an approved protocol for APS patients yet. It’s all trial and error. It’s very lucky if you find what gives you the quality of your life back. ( and yes- it may change with time for some patients. Not all by any means.)
Thank you Tofino5 for letting me add to your post.
I just know that many people worry about NOACS/ DOACS are not recommended... so I didn’t want you to have to explain yourself to anyone!
Others on here are also on rivaroxaban or Apixiban and doing ok under a watchful eye.
Every now and then when they mention it, someone comes on and will tell them that they should not be on it, etc... not realizing you have a special circumstance.
At this point, Tofino5, ozchic, Raw57, and others I’m forgetting - and me, myself and I are something of experts of failing warfarin for some reason or another, despite our and our physicians best efforts.
It’s absolutely maddening....
We try this , that and the other and hopefully find the magic cocktail eventually.
( and like all magic cocktails... sometimes it needs to be treated with time...a bit more of this, a little less of that... and also like magic cocktails, if we get it wrong we can feel tipsy...)
I am currently having INR fluctuations and thought unrelated bowel twisting requiring hospital admission and nasal tube in Feb. And again this week. INR up and down yet symptoms felt like down with TIAs etc. CATscan shows growth on Adrenal gland INR going crazy. Oncologist/ Hemetologist and Urologist deciding growth may be cause.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.