I posted earlier that I had to ask ChatGPt "who came up with the 'gasoline on a fire' characterization regarding the relationship of testosterone and prostate cancer" and that Chat GPT had answered -- Dr. Patrick Walsh -- (father of the radical prostatectomy.)
In that post, discussion turned to Walsh's book "Surviving Prostate Cancer" which I have found to still be a good discussion of the many complexities involved in understanding and treating PCa.
Walsh's book is the source of the scanned and attached Kaplan-Meier plots I want to share in this post because (if I am reading them correctly) they are so startling in their conclusions that they might still inform current patients whether locally advanced or metastatic.
(I was surprised that Walsh even included these plots in his book.)
The plots show the survival times and profiles for two groups:
* men who underwent orchiectomy and
* men who "delayed", got a placebo, and did nothing until some type of "progression" and then underwent ADT
==========================
NB: This is the caption-text which got blurred in the scan.
I broke the text into a,b,c.-- I think I understand a) and b).
But c)? I have no idea what he is talking about, if you do, please post your interpretations.
-----------------------
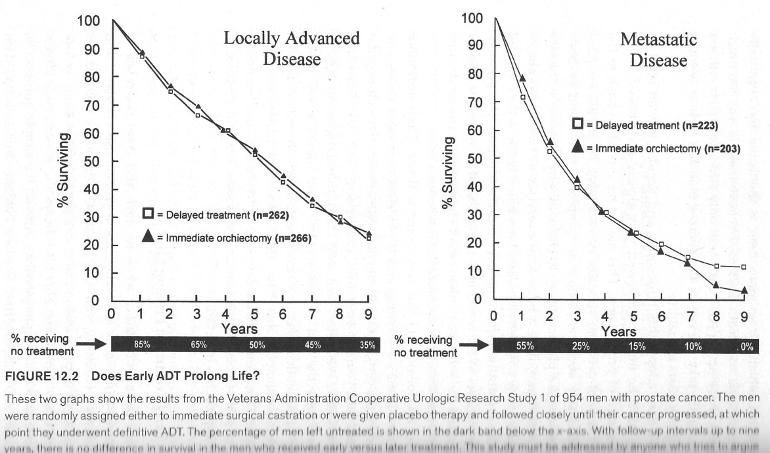
Page 408: Figure 12.2 Does Early ADT Prolong Life?
a) These two graphs show the results from the Veterans Administration Cooperative Urologic Research Study 1 of 954 men with prostate cancer. The men were randomly assigned either to immediate surgical castration or were given placebo therapy and followed closely until their cancer progressed, at which point they underwent definitive ADT.
b) The percentage of men left untreated is shown in the dark band below the x-axis.
c) With follow-up intervals up to nine years, there is no difference in survival in the men who received early versus later treatment. This study must be addressed by anyone who tries to argue that early ADT prolongs life - because if it does, then what's wrong with this carefully executed, long-term study of almost one thousand men?
-----------------------
==========================
Here is the message of the plots as I see it.
The shape of the curves are almost identical for both groups-- so no advantage to orchiectomy.
The men who got the orchiectomy may have believed that their troubles were over. Not only had they eliminated the "gasoline", they had eliminated the entire "gas tank." But they did not survive any longer despite their sacrifice. Their curve "should have" plotted higher and longer than it did.
The men in the 2nd group delayed and did nothing, and so postponed the consequence of the complete castrate-level suppression of both testosterone and estrogen (at least until they started ADT.) In fact it was five years before even half of them needed or received any treatment at all.
And at the end points:
For the locally advanced- 35% never needed or had any treatment over the nine years.
For the metastatic: the delayed treatment group from four years onward still managed to out-survive their castrated brothers.
Have I interpreted the curves correctly or did I make some mistakes?
I see this plot as a metaphor for standard treatment, repeat this "experiment" with different participants and you will get similar results. The numbers will be different in each case but they will be roughly the same as well as the conclusion-- "sometimes nothing can be a real cool hand."
Now let's go out of the box... suppose we could substitute radical prostatectomy for the orchiectomy, would there be any change in the plotted outcomes or conclusion? What about any of the other "local" treatment that SOC forces you to endure before allowing the treatment that works best -- systemic hormone therapy?
And the reason for the superiority of hormone therapy?
Because prostate cancer is metastatic from its inception, way before it can be detected or show up on any scan or even DREs.
Doubt it? A series of men were on the operating table awaiting the start of their radical. Bone marrow biopsies were taken, and found that more that half of them already had prostate cancer in their marrow.
