HealthUnlocked will undergo site maintenance on 8th April 2025 from 11:30AM (BST) / 6:30AM (EDT) for a few hours. We aim to restore the full service as soon as possible. Learn more
Early Estradiol PATCH paper (2008) - Advanced Prostate...
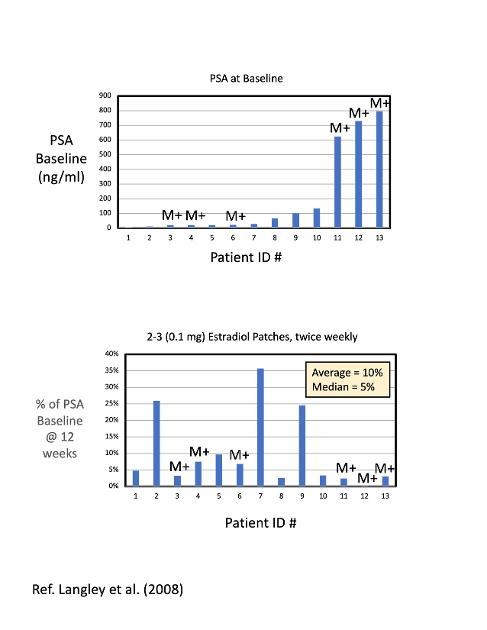
For those of you who have been following the excellent results supporting estradiol patch ADT from the PATCH phase-III trial, I recently ran across this early 2008 PATCH paper by R. Langley et al.
While the numbers were very small for this initial Phase-I study (only 13 men with advanced prostate cancer), six of the men were metastatic (M+). While the results are not statistically significant, this small early study found that the 6 men with metastatic disease could reduce their very high baseline PSA levels (600-800) by more than 95% after 12 weeks of using 2-3 simultaneous E2 patches of strength = 0.1 mg, applied twice weekly for E2 ADT. Their 12-week PSA values ranged from 0.6 to 24 for the M+ group.
These non-significant, early results raise the interesting hypothesis that estradiol patch ADT may be equally effective for metastatic, hormone-sensitive men as for non-metastatic, hormone-sensitive men. Only a few, very small studies have looked at estradiol therapy for castrate-resistant men.
The Phase-III PATCH trial results for a subset of metastatic men out of their total group of over 1000 men with "Advanced Prostate Cancer" may be reported sometime in 2025 after their large dataset has been analyzed.
I have a .pdf of the 2008 paper, if you would like a copy.
Bob in New Mexico
Written by
janebob99
To view profiles and participate in discussions please or .
I really appreciate the details of the estradiol studies you keep coming up with
Thank You
I talked my onco into a prescription of estradiol, she wrote one up for a 0.05mg patch once a week. The reason I wanted to try the estradiol was for anxiety I developed when going from a 3 Mo lupron shot to a 6 Mo shot, I somehow equated the anxiety with female menopause and went through the reviews of estradoil at drugs.com and elsewhere for menopausal women which convinced my to give it a try, I told my onco I wanted it for hot flashes, placebo effect or not I have to say since then I have no right to feel as good as I do.
I read a couple of months ago about your concern with something to do with the E2 receptors that‘s way over my head as are most papers on PC and came to the conclusion that I’d continue to take the risk because I feel so good
Once again thanks for posting the updates on the estradiol studies
That's a good starting dose. You can always increase it later after you can show your MO that you're tolerating it well.
You may experience some breast tenderness and nipple sensitivity. That is common.
The estradiol patches will also help prevent osteoporosis, which is a common problem with Lupron ADT.
If you would like to get occasional articles about estradiol and PCa, send your email address to janebob99@lobo.net, and I will put you on our list of about 12 guys that are taking supplemental estradiol for PCa.
Estradiol patches are used by post-menopausal women to treat hot flashes and reverse osteoporosis. The PATCH study has proved that men can also reverse their ADT-induced osteoporosis by using estradiol patches. The osteoclast and osteoblast cells are basically the same for either men or women, So I would expect that increasing estradiol levels in men without PCa would have the same beneficial effect on bone density as men with PCa.
Thanks Bob! I should sen you a link to a series of videos by a former surgeon who now apparently spends all/most his time withfolks seeking help for their osteopenia/osteoporosis. Exercise, diet, itamins, etc ...plus SOC drugs when those aren't enuf. Mayabe you've already happened upon his videos? I believe I recall that he has discussed estradiol, but very vague memory of that. Evidently there is a reason that some number of women are averse to estradiol? My young Memorial Sloan trained RO would not go along with myask about using that while also using Eligard for my 4+5 RT +ADT. He mentioned the posibility that there might be yet unknown ynfavorable interaction if estradiol were added. Is PATCH conclusively proving that such interaction does not occur. I'm somewhat reticent about striking out on my own, having a treatment failure and then having my Doc assk why I didn't follow his advice!
I have a prescription for Fosamax/Alendronate, but have delayed using it!! Here is that link....
There are only infrequent opportunities withing 100-160 miles of our home to have an Echo light Mers scan done @ $225 OOP. I think I will make a trip for that in March 1st availability at 100 miles to avoid the 160 mile trip to Bend, the home of the machine!! Hopefully another 2 months of waiting will not be a make or break decision!!! Perhaps I overly fear possible side effects of the SOC drugs?
The 14-year PATCH study was a head-to-head comparison between LHRH drugs like Lupron for ADT, compared to Estradiol ("oestradiol" in the UK) patches for ADT, or men who had Advanced Prostate Cancer. Combinations with other drugs were not studied. Estradiol ADT works on exactly the same biochemical/hormonal pathways as Lupron ADT. So, if combining Lupron with another PCa drug doesn't create any bad synergistic effects, I would expect combining transdermal E2 with another PCa drug would also not create any bad synergistic effects.
I expect the PATCH team will be studying combining tE2 with abiaterone and/or one of the 'mides (enzalutatimide, apalutamide, or darolutamide) in the near future.
I have been taking Orgovyx for 6 months and also doing estradiol gel for 8 months, and my PSA is now 0.03. I haven't had any hot flashes and my bone mineral density increased 10% over the past 6 months. I do have fatigue and muscle weakness from the low testosterone levels, as expected. And, some gynecomastia and mastalgia from the estrogen.
Decades ago, both men and women took estrogen orally, which did cause an increased rate of blood clots and CVE's. That's what most docs have been taught. But, applying the E2 transdermallyvia patches or gels/creams, prevents a first pass through the liver, which stops any increased incidences of blood clots and CVE's. The safety profile for Estradiol ADT is the same (or better) as Lupron ADT, according to the PATCH study.
Thanks for the osteoporosis link. I will study it. This beneficial effect of estradiol, highlighted by the PATCH team, will likely have benefit a much larger population of men who have osteoporosis that don't have prostate cancer.
Not that I can tell, but my nipples are tender so it might happen, It's been about 5 months since I started on the patch. I'm also on lupron plus a 250mg abiraterone and 5mg prednisone a day
I got something called a Nuclear medicine bone scan, not sure if that's the same thing as a DEXA, the impression said no evidence of metastatic disease, but the PSMA PET/CT found numerous tracer avid lymph nodes present above and below the diaphragm and of course the prostate. Good to hear on the gynecomastia
DEXA stands for Dual Energy X-Ray, and it is an X-ray measurement technique, not a nuclear medicine test. It measures the density of bones at various location in the body. Lupron ADT causes net loss of bone density due to decreased levels of estradiol. Over many years, the resulting osteoporosis can lead to vertebra fractures, among other bones.
My own bone density increased by 10% over a period of 8 months (by two different DEXA scans), which I believe was caused by my use of supplemental estradiol gel.
That's an impressive density increase,I started Estradiol almost 2 years into my lupron therapy, hopefully it will prevent me from snapping some bones. Interesting on the estradoil up take differences on the Patch trial, I put my patches as recommended in the box literature, I haven't tested my levels
I was following the patch trial. Tried estradiol daily - transdermal for two years and went off Lupron. My PSA went from being undetectable to 2000 over those two years and I developed a skull base lesion (small tumour on my clivus) it took out my 6 th cranial nerve then when that nerve palsy healed up it took out my 3 rd cranial nerve both in my left eye and I got ptosis.
Perhaps I didn't use big enough of a dose of Estradiol. However needless to say I am quite disappointed with the results as I now have constant lingering headaches due to that skull base tumour.
The PATCH study found greater than 90% of their me achieved castrate T levels (T<50) using E2 patches instead of Lupron ADT. But, that means that < 10% of men did not achieve sufficiently low T levels to adequately reduce PSA.
What strength and how many of estradiol patch(s) did you use during that time?
I was using transdermal gel. It comes with a little plastic stick like a ruler with a groove in it. One is supposed to squeeze a bead of gel into the groove (about 3 or 4 cm long).....twice a day. I'm not sure in mg exactly how much it was. I did it off my own initiative. Not supervised by any doc though I told my oncologist that I was using it.
Yes, it may have been too low a dose. Do you know what the concentration was of estradiol in the gel ? It's likely in the range of 0.06 % to 0.1 % (for EstroGel and Divigel, respectively).
The estradiol gel that I take is a much higher concentration, 1.0%, made by a local compounding pharmacy for about $ 1 /day.
Do you have any hot flashes or osteoporosis on your current treatment?
Have you had a baseline DEXA bone density scan?
Did you have you blood levels of estradiol measured?
Interestingly, in the PATCH studies, the range of estradiol serum levels varied from 90 to 580 pg/ml, for nominally the same number and strength of E2 patches. This reflects the tremendous variation in an individual's response to supplemental estradiol . This could be due to differences in Body Mass Index (BMI), age, location where the gel is applied, etc.
I have found research that says a similar, small steroid molecule (hydrocortisone) was absorbed very poorly on the forearm, compared to other locations on the body (which can be as high as 40 times more absorptive than on the forearm).
Wow thanks for that ....a no in answer to all of your questions...only that adt (Lupron) gives me bad hot flashes. That one of the reason I stopped it. I was rubbing the gel on my inner upper thighs and sometimes at the base of my spine on my back. I wish I could find a way to get the 1.00 % gel you mentioned. I don't think there are compounding pharmacies in Malaysia that would do that for me.
I'm just a poor guy trying to survive. The estradiol was much cheaper than the 3 monthly injections.
I'm still interested but at the moment I'm back on the Lupron. I can't afford Zytiga or chemo. Or anything else. The cost of the Lupron injection is about 100 euro a month (I'm not sure in dollars USA ) that's all I can afford at the moment.
I'm prepared to accept that I may have to suffer a lot in the future. I pray 🙏 daily and ceaselessly - I believe God is in control.
No one should have to suffer from Prostate Cancer today.
I believe you can get estradiol gel from Thailand.
You may also want to look for a compounding pharmacy in Malaysia, or another country. The cost of 1% E2 gel is almost the same as 0.1% E2 gel, when compounded. The 1% gel is only about 5-10% more expensive, because the main cost is labor to prepare the mixture. The E2 itself is very inexpensive.
The best locations to apply E2 gel are to the jaw line and scrotal skin, according to Feldmann et al.
According to a different study, serum E2 levels increased by 300-400% when the E2 was applied scrotally, as compared to forearm application,
I currently apply E2 gel to my scrotum, and my serum E2 levels are high (300-500 pg/ml). I don't have any hot flashes (even while on Orgovyx for 6 months), and my bone mineral density actually increased by 10% over the past 8 months of E2 use, according to a recent DEXA scan.
I pay $1 US/day (out of pocket) for my estradiol gel here in the US, compounded locally.
Another study I found showed that the estradiol gel should be applied to as small an area on the skin as possible. That will significantly increase the total amount of E2 that is absorbed. I know that it doesn't make sense, but that's what the study found. Skin permeation is a complex process...
My PSA is now down to 0.03, and I expect the next measurement to be even lower.
The 14-year PATCH study showed that more than 90% of men could reduce their PSA to the same low levels by using transdermal estradiol ("oestradiol" in the UK), compared to men that used Lupron ADT, with no increased rates of damaging cardiovascular side effects.
You may want to drop the Lupron and use your 100 Euros a month to buy estradiol patches or gels. You will need to measure your serum E2 level, and try to reach at least E2 =200 -250 pg/ml. Otherwise, you're shooting in the dark without making some measurements.
Our estimates are that using a high-concentration of E2 gel, applied scrotally, will cost about a factor of about 1000 times less than using depot injections of drugs like Lupron, or pills like Orgovyx, while having the same impact on PCa, and with a similar (or better) safety profile. That's why it's an ideal method for men living in countries that don't have a strong national health care system, or for individuals that don't have a lot of money.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.