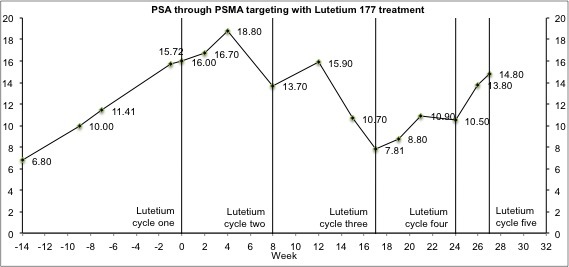
No long story this time round. I’m going to cut straight to the chase. The Lu-177 treatment has stopped working. My PSA has been on a steady increase for the last three months (see the chart). My last PSMA scan showed the large mets in my spine have stabilised, but not improved. Smaller mets in my spine, clavicle and scapula have improved slightly, as has activity in a lymph node.
I had a chat with my Doctor yesterday, after the 5th infusion, and he told me a sixth cycle was unlikely to resolve/significantly reduce the mets in my spine. When I asked him if I should pay for a sixth cycle or spend the money on a family holiday, he said “That’s a very difficult question to answer”.
So, it looks like I’m going to have to try to get myself on an immunotherapy trial. I’m germ line BRAC2 and my tumours exhibit micro-statellite- instability, so there is at least some chance immunotherapy will work. I’ve decided against Cabazitaxel, as I don’t want to feel sick for months for no real gain.
So, my fellow warriors, if you have any advice for future treatment, please let me know. I’m open to pretty much anything. Any advice will be gratefully received.
Aside from that, I'd like to wish you all happy holidays and good/better health for 2020.
I'm curious, why only three weeks between cycle 4 and 5, versus about 8 weeks for the other cycles? You seem to get a spike 4 weeks after each cycle, followed by a drop, so I'll be curious if you do get a drop after your last infusion.
I agree it looks like it's time to move on, but being only at the start of my journey I don't really have any great advice. I do hope, whatever you end up doing next, you get one of those exceptional responses that will give you many more years.
Wow, 17 years. That's both impressive and daunting. Has that time included long periods of disease stability?
Thanks Tom. They brought it forward because of the blood tests and testing people around a machine shut-down/Xmas. I had four and a half great years on Abiraterone.
Thank you Nalakrats. I’m 54 living in London, alternating between private clinics and the Royal Marsden. I’ve had Olaparib, lots of chemo, abiraterone, enzalutimide, Radium, et al. Everything, in fact, apart from immunotherapy. Just trying to decide which type, or if I’ve missed anything. Appreciate the reply. David.
in reply to
54 -17=37 ..... I hate to say it but that’s a hell of row to hoe. You’re amazing what you’ve been through . I’m blown away .. by you... I don’t have any treatment advice . However I Hope love shins on you during this vast journey . You really seem to be a steady person . Admirably strong . 🙏
in reply to
Thank you Lulu700 - and may they shine on you too.
Hello David, I have been awake since 3:30AM here in SW FL and must say that I was deeply affected (saddened) when I logged in and read your post. I CAN NOT offer any wisdom as so many here can because I am a relatively recently diagnosed GL10 taking an alternate direction for my treatment that I AM SURE most would say is STUPID and as such not privy to what many with even lesser numbers are experiencing.
Please accept my heart felt desire that you find a resolution providing a halt to advancement, some comfort and peace of mind *ASAP!!!*
COLD FULL MOON celebratory bike ride for me beginning at 5:17PM this afternoon for the moon rise then biking too see the 12:12AM the Cold Full Moon tomorrow and then until the 7:15AM moon set. Should be an interesting 14+hours of riding, or as much as possible. 125 to 150 miles
BTW, I AM one of Dr. Onik's non FDA approved immuno (alternate direction) patients for my GL10. It's a *wait and see* game. Had PSA and Testosterone test draw yesterday and got my bi-weekly Testosterone injection a few hours ago.
Dr. Onik directed his treatment procedure performed by a physician friend while on a LOCAL instead of a general. The video WXYZ123 mentions is very interesting.
He does a procedure that is not yet FDA approved with approved immunotherapy drugs that’s had full remission for some men. Google him and watch his two YouTube videos
ONIK s a radiologist. My concern in reading you article is how he could be giving treatment in the US that have NOT been FDA approved. I saw his bio and also wonder how he is involved in immunology treatments, as a very different speciality.
That said, if it works, then we ALL need to hear about it, if it just yet another pull of smoke, we also need to do that as well, because, for far too long, men have been used as pawns by those less than scrupulous.
So I am many others wait. If this reaches men who have undergone his treatments, please let us know asap. thanks
You've been through almost everything. Maybe a different PARP inhibitor (like Rucaparib, Talazoparib, or Niraparib) combined with Keytruda (approved for MSI-hi) seems ideal for you. Insurance will cover Keytruda, but clinical trials for PARP inhibitors will exclude you if you've already tried one. I expect they will get approved within the next couple of years.
Have you tried Zytiga with a different steroid, ie., switching from prednisone to dexamethasone? That worked for my husband. Also, I read somewhere that higher doses of dexamethasone alone, as a single therapy, can work for a while.
There are several articles about this. I just did a quick search and found this one:
> There has been discussion about Fenbendazole (dog de wormer) and we found out that Fenben disrupts Micro tubules of cancer cells causing mitochondria to burst resulting in cancer cell death (fancy word is apoptosis)
>
> Niclosamide is an old tapeworm drug still used in most developing parts of the world in children who have tapeworm in their stomach and intestines.
>
> Niclosamide is in news as a re proposed cancer medicine because it kills cancer cells by an entirely different mechanism than fenbendazole.
>
> Cancer cells are deficient in a gene, called p53, which is a tumor suppressor gene. Researchers found out that Niclosamide selecively attacks and kills cells which lack the gene p53. Niclosamide causes accumulation of a fatty acid called Arachidonic acid in cancer cells causing mitochondria to release a molecule called Cytochrome C which ends up killing cancer cells.
>
> A clinical trial is on in UCLA Davis where they are combining Abiraterone and prednisolone with Niclosamide to see its effectiveness.
>
> Ideas and opinions are invited about Niclosamide and its cancer killing potential
>
> Also, please share any personal experience with Niclosamide..
>
>
> tango65
> tango65
> in reply to LearnAll
> 16 days ago
>
> The study a UC Davis uses a niclosamide that is different from the niclosamide used in the trial at the UW Seattle. At Davis they use PDMX1001/niclosamide. This compound made by a Biotech company in Sacramento is absorbed by the gut and makes possible for niclosamide to reach anti cancer levels in the blood. Regular niclosamide is poorly absorbed by the gi tract to reach anti cancer levels without using toxic doses.
>
> clinicaltrials.gov/ct2/resu...
>
> Besides the anti cancer mechanisms you outlined, PDMX1001/niclosamide can resensitize the cancer to abiraterone and enzalutamide They have shown in vitro that niclosamide can revert mechanisms in the cancer cells which make the cancer resistant to abi or enza.
Do you know if it is possible to get PDMX1001/Niclosamide prescribed outside of the clinical trial?
Hi JLS1,
I did the switch with Dex and Pred and got anther year out of Abiraterone.
Thanks for the other info - I’ll check it out. Saw this on the forum a week or so ago then forgot about it - so a good reminder. Will circle back with any results. Thanks again. David.
You wrote: "I’m open to pretty much anything. Any advice will be gratefully received." So let me mention this:
Recently I did some research regarding the use of DES (Diethylstilbestrol) as hormonal therapy. In the following review tandfonline.com/doi/full/10... the authors mention: "The use of DES as a salvage therapy after first line docetaxel-based chemotherapy in patients with progressive CRPC has been studied by a few investigators." They then mention these studies:
Serrate et al. Diethylstilbestrol (DES) retains activity and is a reasonable option in patients previously treated with docetaxel for castrationresistant prostate cancer. Ann Oncol 2009;20:965. academic.oup.com/annonc/art...
Shamash et al. A phase II study investigating the re-induction of endocrine sensitivity following chemotherapy in androgenindependent prostate cancer. Br J Cancer 2008;98:22–4. nature.com/articles/6604051
Cox RA, Sundar S. Re-induction of hormone sensitivity to diethylstilboestrol in androgen refractory prostate cancer patients following chemotherapy. Br J Cancer 2008;98: 238–9. ncbi.nlm.nih.gov/pmc/articl...
"Re-induction of hormone sensitivity" means that DES did work after Docetaxel. One of these studies concludes: "Since there is no standard of care when progression occurs after docetaxel-based chemotherapy in patients with CRPC, DES appears as a reasonable option worth considering in this setting."
How many intervening treatments have you had since Androgen Deprivation Therapy?
Maybe its time to try it again, but this time with Bipolar Androgen Therapy (BAT). You alternate the ADT with very heavy overloads of testosterone.
For some this makes it castration sensitive again. There are Docs in the US who are experienced with this and are willing to do this.
Jevtana is considered second line Chemo after Cabazitaxel. And it has much less severe side effects. Have a discussion with your Doc about its side effects.
Maybe mix it in with that BAT.
Also when is the last time you had a genetic test. Things change. See what a new test gives you.
Hi cesanon, my dad had a very difficult time on docetaxel, and it failed...his doc isn’t sure he’d fare well (he’s 87) enough to do cabazitaxel (though my dad was game to consider it). So do docs ever skip over cabaxitaxel and go to jevtana, or do they firmly adhere to a schedule of the treatments and religiously try them in order?
I am now in year 19, so have been even luckier than you. It is very difficult when one's options shrink, but you have gained a great deal of extra time that many men never and will not have. You have also laid down a framework for others to follow, and at the least, that is someone that we advanced guys can off the next generation of men, who might otherwise die far to early.
I have come to terms myself that at some point, there is no point, and by planning ahead, i.e. my big push for making a bucket List and living large, allows one to approach the end in peace. I have helped many men in their last days, and sadly the end for PC is one godawful horror show. I have prepared my ending in advance, will keep up the fight as long as I can enjoy and do things, but never will I go down that path-i only hope that I have the courage to say goodbye when that day comes.
In the meantime, do as much living as you can, love those close and do good things for those around you! It is not how long we live but how well we live. Take care and go in peace.
Were you thinking about a combo therapy with Lu177 and Actinium 225? Because in the past Lu177 alone seemed not strong enough to treat mets in the bones.
Maybe the combotherapy is less aggressive than act225 alone? My husband had 3 Lu177 shots and took also 4 weeks ago the cholera vaccine Dukoral. We'll see in a few days if his psa is still dropping. He had no bonemets, but Gleason 9 and stage IV cancer, detected in October 2018. And a RP on the 30 November 2018 and than they detected 6 mets on lymphnods and his Psa rose to 4.40.
The last psa test a month ago after the 3 Lu177 treatments was 0.46. Good luck to you.
Where did you read this? As far as I know there is no difference between the I&T ligand and the standard LU177 ligand. The salivary gland expresses PSMA so both ligands will attach to it.
The I&T version was developed at the University of Munich which has the capacity to manufacture it too. I think the clinics are using the I&T version to avoid licensing problems with Novartis which may arise in the future. The I&T and PSMA-617 versions are basically interchangable.
Heidelberg cooperated with a private company called ABX to get the ligand manufactured and this company sold the rights to Endocyte which was bought by Novartis a year later for 2.1 billion dollars. Although the Lu177 development was funded by the German state, the patients will have to pay billions to Novartis to get the treatment after it is FDA approved.
Well it looks like you used all the sledgehammers available to you. As a no risk no loss and cheap option why not consider the Lisanti protocol of vitamin C + Doxycycline + Azithromycin. Certainly won't do any harm. Good luck and Christmas greetings.
I read somewhere there are clinical trials for new "targets" for radionuclides, away from PSMA. If I find it (or anyone else here has it), I can share. Hopefully you still have a long time ahead.
That is impressive. You might ask your doctor if he thinks your cancer might have morphed into small cell carcinoma. That has happened to me. They treat it with Carboplatin along with the typical chemos or Toposide, which is used for lung cancer. Something to consider as well.
Wondering if you have considered Estrogen patches?
While my situation is not nearly as complex as yours judging by the train of therapies you have been through.
I am using a relatively high dosage of x4 patches changing 2 each day and it has taken PSA from +24 due to lymph node metastasis to <.008 or unmeasurable and testosterone which apparently feeds prostate cancer is also <0 and unmeasurable .
There was some bad press on Estrogen as female hormone replacement which it turns out was due to a poor analysis and the use of oral rather than dermal therapy.
There are numerous reputable clinical data publications online some of which I gave to my oncologist and he agreed and in response to my positive outcomes he is now using this therapy on other patients.
Just a thought as it has minimal side effects and while in Canada I have to pay the cost (C$200/month) it has less risk of cardiac and night sweats etc. than any other therapy.
BTW I have had both the radical surgery and radiation prior to starting Estrogen
Good suggestion Peter! I have been using Oestrogel (tE2) and I'm thrilled with the results. Richard Wassersug has been using it for about 15 years and his PSA is still undetectable.
I think you would be a good candidate for Lynparza/Olaparib. This is because of your Germaine BRCA2 mutation. They have seen tremendous success - like over 70 percent of patients achieve progression free status. Contact Johns Hopkins. There may be a clinical studs. Good luck!
Thanks - but I’ve already had it. Didn’t work unfortunately. I think the sample sizes were probably too small to be significant if I’m honest. But, what do I know. 😀
David, Please read Petercraig2's reply above. You may also want to read my history with the use of estrogel...basically the same therapy as the patch except that IMO it is easier to use and far less expensive.
17 years? You were diagnosed at age 37.... Looking at my crystal ball computer I figure you'll still be complaining about not being able to ride a bike at the age of 88. Index and Middle fingers to those tiny bastards....
Good Luck, Good Health and Good Humor.
j-o-h-n Wednesday 12/11/2019 8:37 PM EST
No Nal, I Can not. I flipped out with rage because I was early to the stage #4 party I thought at 53...My good man cadence was’nt even middle age yet .. bless him ..He’s a special dude to have survived what he has .I have no right to complain now or about those 52 years that I was never sick . I did take note of one young man of 16 with APC ..That ain’t right.. Take care Nal. Shalom
That has been a major issue. I’ve tried lots of things - injections etc - but nothing has worked that well. If I’d known I’d get 17+ years I would have had implants.
Oh no John, anything but not being able to ride my bikes again! 😀
What a great post so full of ideas for our desperate times! Thanks to all.
My husband is 19 years since diagnosis and has gone through years of maiming treatments. He still enjoys life working two days a week at Habitat for Humanity when I don't have an extended trip planned to keep him from it.
Today, I am on pins and needles waiting for yesterday's PSA results. One would think that after all these years I could just relax and not get freaky.
Husband had an unexpected, amazing 3 point drop last month but we don't know if it's the Zytiga or Fenben or part of the Fenben protocol or the magic of Provenge 3 years ago. Whatever, we will take it, fingers crossed, these are the best of times.
From what I recently read Keytruda only works in a select few people with certain gene mutations and there is difficulty in screening just who will benefit. If you get lucky with Keytruda it can add two years to your life but with potential serious side effects. It almost killed our neighbor who had a terrible reaction to it. He died a shortly afterward.
Nalakrats. Hi based on your post above I believe we nearly crossed paths today. I would have enjoyed meeting you.
I completed salvage radiation this morning possibly at the same location and have a question.
So while receiving that whole pelvic IMRT PBLN +ADT I discontinued taking all antioxidants, I wonder when the right time is to begin taking antioxidants again?
These hormonal cancers are on the rise. Just a sign of the times and the demise of the human race ..
That’s a good point. Could have that as the final cycle - rather than the straight Lu-177 shot. Having said that, I’m a bit worried about the issues pointed out by tall Allen
Could I just ask what your background is and whether you have any links to the German hospitals giving this treatment? I ask because your knowledge is very impressive. Thanks again and happy Xmas. David.
If you respond to the combined cycle this does not need to be your final cycle. I do not know where you got your Lu177 treatments so far, it may well be that they can do the combined treatment if you ask for it. In general if you contact possible clinics you have to make clear that all you want to get is this combined treatment – and not their standard of care. Of cause Prof. Ezziddin in Homburg/Saar who wrote the article I mentioned will do it but he seems to have capacity problems currently. Heidelberg and Munich can also do it. Bad Berka did it as well but Prof. Baum has left now so I do not know how they proceed. You may have to wait longer for the combined treatment than for a Lu177 cycle because Ac-225 is more difficult to get for the clinic.
I am a PCa patient in Germany who does a lot of research regarding prostate cancer. I had one cycle of Lu177 which wiped the lymph node mets off the PSMA PET/CT.
I would not worry about the issues pointed out by tall Allen. I never read any references to repopulation in conjunction with a Lu177 therapy yet. It is probably a very rare occurence that a Lu177 therapy makes things worse, if it happens at all. Patients with limited options left should not worry about this.
As you can see, this patient progressed while receiving Lu177 threatment and after that responded very well to the combined Ac225-Lu177 treatment (=TAT).
On these conferences they always show the most impressive cases. But as you can see, the combined therapy can have a benefit for patients progressing during Lu177.
Andreas Türler presented on different radionuclides and showed this slide which he got from Prof. Baum. Prof. Baum had treated this patient.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.
") Thanks for the reply. David.
Thanks for the reply. David.