In Oct. 2017 I suddenly experienced numbness to the sole of my right foot, within a week I developed severe and debilitating pain to right leg and hip. PSA was at 48. Whole Body scan showed mets to pelvis, lumbar spine and sternum. MRI showed tumor at S1 which resulted in sacral fracture. 15 radiation treatments killed tumor and pain diminished. Oct. 2017 also started on Casodex and Lupron. By March 2018 my PSA had fallen to 2.6. By April 2018 it increased to 5.6. By May PSA was at 10.3 and MO suggested I immediately start Docetaxel. June 2018 out of state family crisis delayed treatment start by four weeks, PSA had hit 16.8. Two infusions later, the end of July, PSA had dropped to 9.4. From 9.4 low PSA continued to rise throughout remaining 4 infusions and was at 30.1 at the time of my last infusion. Oct. 2018 Whole Body Bone scan showed small increase in metastatic disease, (I'll add that scan image in a following post). Two weeks later PSA hit high of 32.6. Mid Nov. I started 1000mg Zytiga with Prednisone . Two weeks later PSA had fallen to 15.1. The drop continued and by Feb 2019 PSA was at 12.2. PSA then rose to 15.6 by March and continued to rise to 19.6 by April 24th. Whole Body Bone and CT scans April 2019 showed significant progression of metastatic disease, with no soft tissue involvement.
In the weeks since latest scans, AR-V7 test came back negative. Foundation One Liquid Biopsy, no reportable genomic alterations detected, (Foundation One tissue biopsy to be scheduled), Bone Biopsy of L3 Vertebral tumor came back questionable according to my MO, as I developed retroperitoneal bleeding which interrupted the procedure and as a result I found myself in Surgical Intensive Care for a day and a half. MO wants me to repeat the Bone Biopsy at another facility but the thought of having a power tool drill into my bones once again is something I care not to repeat.
Currently my MO is searching for a suitable Trial Study, if none are found he is suggesting Cabazitaxel/Carboplatin chemo or Xtandi/Xofigo combos.
I welcome any thoughts or suggestions regarding treatments going forward.
Best to everyone.
Written by
SsamO
To view profiles and participate in discussions please or .
Therein lies the problem. The preliminary pathology comment stated. Metastatic prostate carcinoma is absent. Immunohistochemical studies to evaluate micrometastases are in progress. The final pathology report stated, Metastatic prostate carcinoma is absent (IHC Pan-K, PSA & PSAP negative.)
Immediately after the biopsy It was explained to me that I started to bleed internally once the biopsy was completed. Once in ICU the Radiologist told me the samples (2) he got were good despite the bleeding. My MO upon reading the final pathology report believes that I started to bleed during the biopsy which limited the radiologists ability to determine if the samples taken were viable for testing. MO believes pathology report should have more inclusive hence his reasoning for redoing the bone biopsy. Trying my best to comprehend all of this, I welcome your comments.
It sounds like you do not have normal acinar adenocarcinoma in that tumor - you have some rare type. You have PSA positive somewhere else, otherwise your PSA would never have been that high. They have to figure out exactly what type of prostate cancer it is.
Yes we have talked about that option. Thursday my MO faxed my file to a colleague (forgot his name) at MD Anderson Houston. I'll mention Duke to him when we speak on Monday, I'd prefer the Mid-Atlantic over anywhere in Texas.
I'm wondering if you have the neuroendocrine phenotype of prostate cancer. I'm not a doctor, but seems to me that a PSA of 48 is low for amount of bone mets you show in the bone scan. That would also go along with the short duration of response to ADT treatments. There are some neuroendocrine markers (CgA and NSE specifically) that can help determine if that's what you have. These are blood tests you could have done quickly and without another biopsy. Like your doctor suggested, I think Cabazitaxel/Carboplatin or Xofigo are good choices, but I would be skeptical about Xtandi considering the history of your treatments. These are things you could discuss with your doctor.
Wishing you the best, and please update us when you know more.
gregg57, I appreciate your comments and yes I did mention neuroendocrine PC to my MO, at the moment I can't recall his reasoning but at the time he thought I didn't have that differentiation . I will however question him on Monday on the CgA and NSE blood tests, they seem like a simple solution, and a lot less painful, I'll also ask about Xtandi.
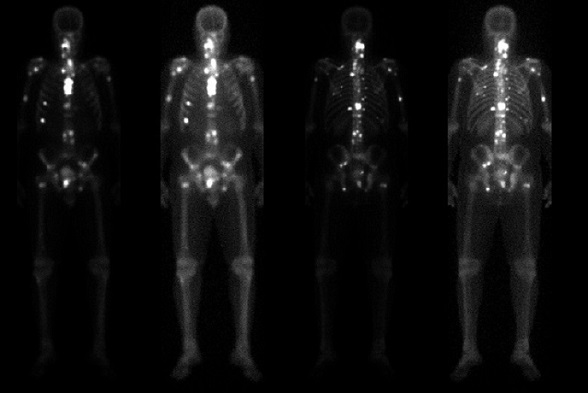
To clarify, back in Oct. 2017 when my PSA was 48 my scan showed only a few mets. The scan pictured above is from April 4th 2019 when my PSA was at 18, and my scan from 6 months prior shows approx 60% less mets. So yes, as my PSA has fallen the numbers of mets has increased dramatically, and my MO has remarked that such a high tumor load for such a "low" PSA is indeed rare.
Thanks again for your thoughts and time. Best to you.
Just curious, have you had your calcium level checked? If so, is it elevated?
Yes, CBC and Metabolic Panel is done every 3 weeks. Calcium is always within range and averages between 9.5 and 10.3.
It would rare to have high calcium levels which can occur from osteolytic metastases. More common in other cancers. Neuroendrocrine cells are also rare in prostate cancer at diagnosis, but become more likely with successful androgen-based treatments just due to the natural selection process. Let us know how the blood tests go.
Well Sam... As you well know we are on opposite sides politically but that doesn't stop me from wishing you well. It appears to me that you don't have someone who's accompanying you when you visit your doctors. If possible get someone to go along and act as a scribe because most of us go into a blue fog when consulting with our doctors. If you ever decide to come east to NYC for consultation with a very competent MO at Memorial Sloan Kettering please let me know. Take care and you'll beat this bastard...
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.