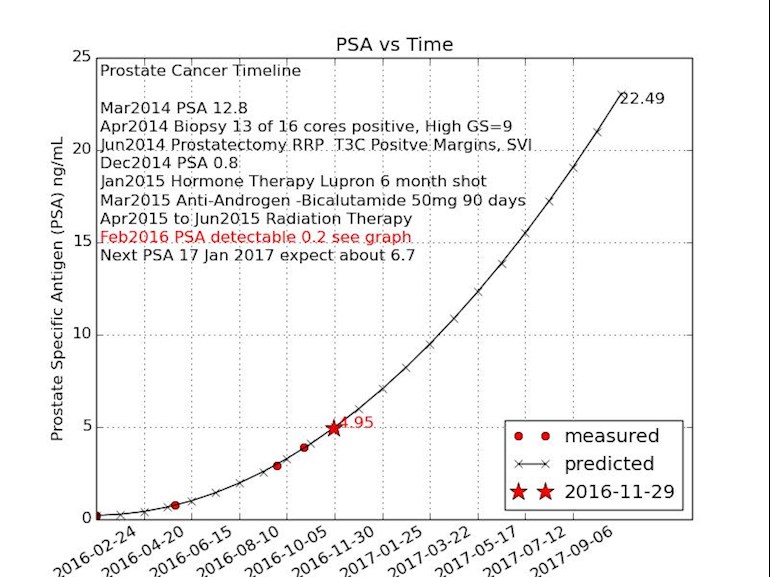
This my first post to a prostate forum. I am 64 years old and have generated a graph (attached) which contains all my pertinent information. PSA, biopsy & prostatectomy in 2014, hormone therapy & radiation in 2015 and an increase in PSA from 0.2 in Feb 2016 to about 5.3 currently. Hopefully the graph and the timeline text explains my status sufficiently. The curve-fit predicted my 4th PSA to within a few hundredths in mid October. The next PSA is scheduled around 17 January and based on the curve, the value should be around 6.7.
I am not sure that I have a question, but as you can see I am bit fixated on my PSA values. My oncologist has suggested that I could start hormone therapy again, but if I do, I will continue it until it becomes becomes ineffective, so his suggestion is to wait until there is identifiable cancer on a scan before restarting hormone therapy.
My apologies if my post is not appropriate for the 'Advanced Prostate Cancer' forum since I am not sure that I qualify.
Yes you qualify unfortunately. As your graph points out your psa doubling time is quite short. I am not an expert but in my experience there is no good reason to delay a return to hormone therapy. The concept of letting the disease progress unchecked until it is shows up on scans does not seem like good advice. If I were you I would get a second opinion from an oncologist who specializes in prostate cancer.
My cancer and treatment history is posted in my profile.
I hope this is helpful
Bill Manning
• in reply to
Bill - Thank you very much for the feedback. It was what I was looking for in posting my info.
I read your profile and you are in my thoughts. I appreciate you taking the time to respond.
I am an electrical engineer working for an aerospace company and my job is to manipulate data, usually time series information, and make sense of it, usually by processing and plotting it. The graph was made with the Python programming language, which I would be happy to share with anyone that wanted it, but it might be a little confusing to those who are not programmers or data manipulators. I am going to try to transfer this to a spreadsheet tomorrow, so that it can be done in Excel or Google Docs(Sheets). It might not have all the text information, but it should allow a user to enter actual PSA results (date, PSA value) and then curve fit it so that you could get an estimate of where you are on currently based on past PSA data.
I agree. I wish you healing and it looks like you are very proactive and organized in your approach which I think will benefit you greatly . get 3 opinions and find 2 that concur along with your own sensibility . it's great that you are so proactive early on. I think the fixation on psa comes with the territory but if you ask me on here they have demonstrated psa changing in the same day and upon charting daily. please someone post the link to the beautiful soul who did this process to benefit pca research.
My RP was in 2004 & salvage radiation in 2015 - 10 years before yours (at age 56 & 57).
My PSA was increasing after each & it hadn't been long since ADT was the knee-jerk reaction. Being youngish then, I was fearful of having CRPC by age 58, with few options if the cancer became metastatic. No Zytega then, or Xtandi, etc.
So far, I have avoided full-scale ADT. ADT is paliative & short-term. Some men have been on ADT for many years, but studies still often start with a statement that ADT mostly fails within 18-24 months. Not only fails. ADT changes the nature of the cancer.
Your graph looks scary, but the 4 points that neatly fit, do not convince me that the next 4 will.
What would I do (& I'm not a doctor ... & so on ...)
1] Inflammation. It affects the PSA doubling time. It can be controlled. Test your serum albumin & C-reactive protein [CRP].
2] Coagulation. It affects metastasis & needs to be controlled. Test your D-dimer & fibrinogen.
3] Hormones. They can affect progression IMO. Test estadiol, testosterone & DHT.
4] Metformin. Dr Myers recommends it.
5] Statins. What were your latest lipids numbers? Include triglycerides.
6] Metabolic syndrome. Do you have any of the symptoms?
7] Diet. What % of fat do you eat in a normal day?
8] Antiandrogen. Consider Casodex.
9] 5-alpha reductase inhibitor. Consider Avodart.
These are just discussion points. Some require lab results.
Written in haste. Apologies!
-Patrick
Hi Patrick - I just spent over a half hour trying to reply to your message. I basically have to google almost every one of your discussion points, since I have a very low level of knowledge on each of the points. I appreciate the feedback and will respond more appropriately tomorrow.
I do agree that the four measured PSA points in 2016, do not at all indicate what the next four will be, but I am only trying to get to the very next one on 17 January and see if it is higher or lower than my prediction from the fitted data. I am expecting a PSA of 6.7 on 17 January. At this point I would get a PSA test every week if my insurance would pay for it, but since it won't, I am using this to keep me occupied
Thanks for all the points of discussion. I can see that I need to become more knowledgeable in order to keep up with the discussion on this forum!
Lyle
• in reply to
Lyle, I’m sorry, but you ( are) as qualified as anyone else here unfortunatly . Waiting for something identifiable to take action does not seem kosher....Before long ,you’ll have more info on this subject then you could have ever imagined.If possible get an opinion from a prostate cancer specialist. Hopefully you will get that PSA down to 0 for many years to come. It is possible .I know because I’ve been >.o4 for 3yrs with Adt & radiation. I have no visible signs for now with a projection from my specialist that within 4 yrs it will return. Just because they can’t see it doesn’t mean that we are clear. None of us can say that. .We plan to push this baby back as far as possible .You can also. Please enjoy this holiday Season....Then after, let’s get that chart going in the other direction.
Lyle, you are in the right place. grateful to all these men teaching me so I can help my dad.
You have had your prostate removed and the prostate "bed" radiated (plus ADT). Still you have prostate cells that are creating PSA. You say you dont see where they are on the scans. I assume these are T99 Bone Scans, and CT scans. There are better scans available that will tell you where the mets are. I would not want to "wait" for them to get bigger if there was a way to see them now.
I also think that you should move towards getting back on ADT, at least until you can come up with a better plan.
Do you think the mets are bone mets or lymph node mets?
• in reply to
Hi
Thanks for the reply. You have described my situation accurately. Yes the scans that I have had so far have been CT scans and Bone scans (not sure if they are T99). I would be interested in more information about better scans than these. As to whether I think the cells are growing in my bones or lymph nodes.... I haven't a clue. I have had zero pain associated with the prostate cancer over the last 2 1/2 years. I hesitate to attribute every every twinge I have to the cancer. I do have some consistent very slight pain (not even aware of it during the day) in one of my left ribs.
It seems like the consensus here is that the 'wait and see' strategy is a loser. I know my oncologist would put me on ADT if I requested it.
I truly appreciate your feedback and suggestions. Everyone has been very helpful. Thank-you
It's good that you are concerned and that are following this closely. If the PSA continues its predicted path, you may want to consider taking actions that involve more than suppressing the cancer. In my own case, I watched and waited for 2+ years watching my PSA go up like yours and having four biopsy procedures. When my PSA reached 11 and then 13 over a period of six months I had a pelvic MRI and a lesion was found that subsequent biopsy analysis rated a "4+". My Gleason Score was 3+4=7 and I chose to act while the cancer was still contained in the capsule. I chose IMRT radiation over prostatectomy and am in my 28th of 42 RT sessions. I should know about "success" 3 or 4 months down the road.
Your situation is unique to you, but I caution you not to wait too long if you find rapid PSA elevation and a rising Gleason Score. Oncologist advice is critical, but you get to decide. Good luck.
Lyle, I will not repeat what many here have stated-all good advice. Where do you live? Getting a second or third opinion from a very experienced urologic oncologist is a must. They are mostly at academic centers or cancer centers. You are looking at precision in your approach. Since we only get one chance at this, you want to give it your best shot. At 64, you are young and I agree with others that waiting for mets to show up is not in your best interest. This is definitely not a "wait and see" situation with your numbers and your history.
Lyle, I too keep a similar chart to track major events along with my PSA in an Excel spreadsheet. Guess that happens when you are an engineer. You might try Provenge. It's effectiveness is difficult to measure. It sensitizes your immune system. If your costs are covered my insurance, I would go for it. Treatment is typically over 5-6 weeks. If someone would like a copy of my spreadsheet, I would be glad to provide it. Haven't figured out how to paste it here.
Thanks for the suggestion for Provence! I will check it out.
I am going to try to create a spreadsheet in Google docs and then paste the link so that if others wanted to do this for their PSA values they could plot their expected values. Maybe we could work the bugs out together?
I don't use Google Docs. I am an old MS Office guy. I spent 20 minutes or so trying to figure out how to paste my Excel chart here without any luck. Tried converting to pdf, but that didn't work either.
Another thing to try is this Sloan Kettering algoritm to track your PSA doubling time. This is more useful than just your PSA tracking. mskcc.org/nomograms/prostat...
Thanks for the link and to martingugino for catching the extra period at the end.
I am attaching a link to the python script that generates the graph in python.
I can see that there are a number of people that might want to use this, although you do need the Python programming language installed on your computer to run it. It is just a text file and can be opened in Wordpad but to make it generate the graph you need Python.
You have aggressively dealt with your PCa with RP, Rad and ADT treatments. You didn't say where your mets were when you rad and adt them. So did your onc scanned the same areas if they're re-growing there? Did you bottomed out to undetectable when you stopped treatments? Or 0.2 psa your bottom?
With a rising psa given a history of mets, I also question why not be aggressive again. Scan technology is not up there yet where it'll glow on micro mets. I had all types of scans after rising psa from .5 to 7.8, and the only one that showed a suspicious area was mri with colorectal coil. Or the radiologists for the other scans didn't spot them. So if you must I suggest mri with colorectal coil around the pelvic area.
Now, f you had lymph node involvement, there is that possibility that PCa cells have travelled into your circulatory system and that would be near to impossible to detect via scan. CTC biopsy may detect it if numerous enough. Fortunately, we can be guided by psa numbers. I'd say you need an onc specializing in PCa and hematology.
I wish you the best. PCa is one hard Ca to treat after it had met. We're in this together and you're in the right group. Take care my friend.
Welcome to the club / forum. I am a retired 66 year old EE. I've written a few python scripts myself. I am early in my journey. I had a modest PSA of 2.7 when I was diagnosed a few months ago. I had HIFU surgery a couple of months ago (so my prostate is still there). I will be getting the results in Feb and hope that I don't join the rising PSA club. There's plenty of valuable advice and support to be found here.
All - I am overwhelmed at all the comments. Thank you!! I probably should have chosen a better time to join this forum. My wife had a full knee replacement today and I have been going full tilt all day, with only a quick read of most of your comments. I will put more time into your comments and responding to them in the upcoming days. I may be a little slow in my response but it is not because I do not appreciate all of the feedback from the group.
As far as being qualified to be part of the Advanced PCa forum, it reminds me of story that I understand that Lincoln told about the man who was tarred and feathered and carried out of town on a rail. A man in the crowd asked him how he liked it. His reply was that if it was not for the honor of the thing, he would just as soon walk.
I feel the same way about being a member of this group, if it was not for the honor of the thing I would just as soon not have made the grade to be a member.
I will comment only on the latest scanning technology:
1. For bones, get a Sodium Fluoride F-18 PET/CT
2. For soft tissue, get a C-11 Acetate PET/CT at Phoenix Molecular Imaging.
You need to locate your cancer in order to develop the best treatment plan.
Never Give In!
Until you know where the cancer is, there is another category of things that can be done to your whole system, besides ADT, which is in the "hormone" category of systemic treatments. Lots of options, btw, in the hormone category,
Provenge, as was mentioned, is in the immunological category. There may be clinical trials in that category. These would mostly be Provenge plus something else, and could easily be interesting and to your benefit. Researchers are often wanting to get their hands on someone like you. A newbie, shall we say, with a nice ECOG score. People could easily guide you to options that could look reasonable for you.
The focal, or localized, therapies depend on knowing where the cancer is, so have to wait, for now.
As for Provenge, here is a little video from a conference in 2014 about it. Chuck Drake is one of the the leaders in the field. youtu.be/2FtHcVJnOgk
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.
")