Just met with my GP this morning to review my current symptoms, dosage and request for additional blood tests. I continue to be in awe of how co-operative he is being!
He agreed to all my request for tests, although I may have to pay for FT3 because of the provincial guidelines that essentially tie his hands.
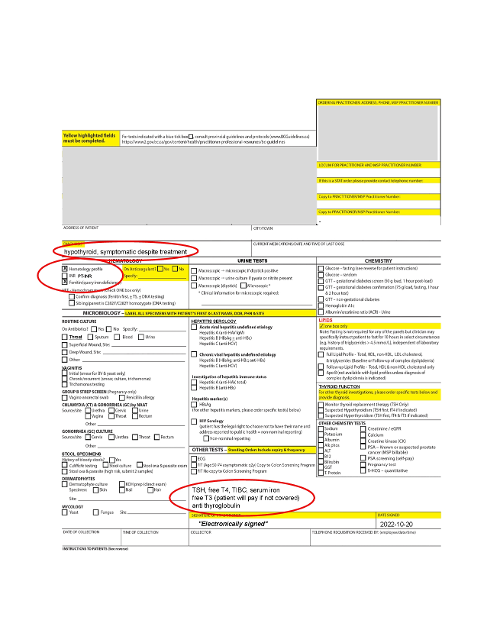
He requisitioned TSH, FT4 and FT3 (with a note that "patient will pay if not covered"), a full iron panel as well as hematology panel and ferritin (due to me having lost half my hair and to see how much longer I need to supplement to reach normal levels). He even ordered TG-ab even though TPO-ab were negative -- although he thinks (as do I) that it is wise to assume it is Hashimoto's and act accordingly when it comes to diet, increased risk of other auto-immune conditions.
I am going for blood tests Monday, should have the results back in 24-48 hours and am meeting with my doctor again next Thursday. I will keep you posted on the results.
I explained my reason why I wanted FT3 tested (i.e. assess conversion from T4 to T3) and will be faxing him two studies by JE Midgely et al (Variation in the biochemical response to l-thyroxine therapy - peripheral thyroid conversion efficiency - 2015, Time for a reassessment of the treatment of hypothyroidism - 2019).
Surprisingly, my doctor knew about the conversion of fT4 to fT3 having been measured in T4 only-medicated individuals (!) but he wondered if the data from those studies can be used to evaluate conversion in those (such as myself) who are already on T4/T3 medication. Can anyone (including diogenes ) speak to that? Are there any papers I can share with my doctor in that regard?
I am both thankful and very mindful that so many others do NOT have doctors like I do, that are willing to learn so they can effectively treat their patients. He is almost retirement age, so I have HUGE respect for him.
Written by
Joyya
To view profiles and participate in discussions please or .
Joyya you can only look at conversion if you are on t4 only. When you are on combo t4, t3 the ft3 level becomes dependent on your dose of t3 and the interaction and effects taking t3 has on TSH and on ft4 levels . For example taking t3 tends to lower and suppress TSH. Tsh has an influence on conversion so by lowering your tsh with t3 you may affect conversion slightly.
ft3 levels are a result of conversion of t4 as well as how much t3 you take when on combo. But because of all the interactions you cannot determine how well you are converting that is only possible on t4 monotherapy.
Can you point to a reference (academic would be most helpful) as to what the optimal ranges are for TSH, fT4 and fT3 are for those taking medication -- and is it different for those taking T4/T3 combos, and if so can you point me to a reference as to what those should be?
what I meant was, what levels of TSH or fT4 or fT3 would be concerning to my doctor? I have read that TSH between 2 and 2.5 is okay for those on medication and can support that from the literature to my doctor, but is there anything in the literature to support acceptable fT4 and fT3 levels for people on T4/T3 combo?
6 weeks ago, I was on 40.5 mg desiccated bovine thyroid three times per day (estimated from papers of analysis to be ~73 mcg T4, 15 mcg T3 per day)
My TSH after 6 weeks on that was at 3.47 (0.32-5.04) and fT4 was at 14.0 (10.6-19.7).
I am currently taking 75mcg of Synthroid and only 10 mcg of Cytomel (so theoretically less T3 than before).
Will synthetic T4 & T3 really suppress TSH that much more than NDT of *approximately equivalent* T4 and less T3. I know the calculations (NDT to synthetics) are theoretical.
I am still so tired and have many other residual symptoms, I really don't want my doctor freaking out.
This may seem like the wrong approach, but what can I do between now and Monday to cause less suppression of TSH?
but what can I do between now and Monday to cause less suppression of TSH? .....
nothing. ... (the only thing that might possibly influence TSH in that short a time would be to stop all levo and T3 today.. which would obviously be a very bad idea from your body's point of view. .. and even then, TSH may still not have enough time to react .. it can be very slow to react ~ hence the minimum 6 week wait for blood tests after any change in dose. TSH test is in effect a window into the recent past ie a measure of "what your hormone levels have been in recent weeks" .. whereas fT4 and fT3 tests are a measure of "what your hormone levels are today" .. so trying to manipulate TSH test results to please a doctor is a pretty pointless task . usually the only way you can do it is to make yourself rather unwell , which defeats the object.
i wouldn't worry about what your TSH will be at the moment ... your Doc sounds quite reasonable... and even if TSH is very low and he freaks , you can always ask to wait for a repeat test after another few months once current dose has had more time to settle .. 6 week is really the bare minimum to asses bloods (and symptom response)~ TSH (and fT4 / fT3 and symptoms ) will often change further once a dose has really settled in .
As your TSH was still relatively high on that dose of NDT .... and now you are getting less T3, (theoretically) , there is no reason to assume your TSH will now be extremely low just because you have switched to synthetic T4/ T3.
just see what it is on current dose and how Doc reacts and go from there. , remembering that 6 weeks is the minimum and further changes may still happen .
I’d like to chip in. TSH is terribly unreliable as a measure. As tattybogle has mentioned, it’s not real time. We know it is an indirect measure. There are numerous factors that can render it unreliable, including issues with the H-P-T axis. From first principles it really doesn’t make sense putting so much ‘weight’ on the TSH measure and I’m always baffled- where is the scientific rigour?
Can’t remember if I have shared my analogy that I made up to get it clear in my mind.
The neighbour analogy. So I want to know how you are and I decide to go and ask your neighbour. Depending on your relationship with your neighbour, I could get anywhere from ‘I do not know’ to ‘oh yes they’re okay I saw them a few days ago’. The question has to be asked - if I wanted to know how you were, why wouldn’t I come and ask you directly? Quality of information from your neighbour can never be as reliable as asking you. 😊
There is absolutely no logical rationale for using TSH to dose patients. The real deal are your actual thyroid hormones and even more importantly symptoms as there is no one size fits all. It’s as unique as a finger print.
Being in range is not all there is to it. MANY Doctors think just ‘drop kicking’ you somewhere in range is sufficient. In fact, it is important to get you in the right place (if indeed the range represents your circumstances anyway).
There are limitations to any model and the blood tests with their ranges are no exception (if only the doctors did but know). The most important thing is that your symptoms are considered in conjunction with your test results, not ignored in favour of test results.
Test results should never be prioritised over the symptoms AND they should be calibrating the tests to you, not you to the lab work. We are all different.
So when a person says “oh doc I feel terrible!” and a doctor says “ but I can’t understand it ???? your bloods are fine”That is a classic case of treating the lab work.🙄I’ve been reading round the subject nearly 2 years and slowly getting up to speed and these three issues confound treatment
Over reliance of TSH
Ignoring symptoms
treating the lab work
You are blessed with a good grounding and a receptive doctor- who is almost retiring and has probably been used to using symptoms to diagnose in the past. A seemingly dying art.
I like the neighbour analogy. It's a good way to explain it.
On one hand, my doctor is very helpful, on the other, he needs (? is receptive to) credible information I share with him — especially ones with academic references.
On our Thursday visit he was talking about aiming for T4:T3 ratios in medication of 13:1 because that is what a healthy human thyroid produces, yet reading about ratios of 11:1 and even 8:1 used. I pointed out that porcine NDT is 4:1, and is often used successfully, which he reluctantly agreed.
He is VERY new to prescribing T3 (I'm his first patient, I think, and it's only because I started (successfully) self treating for 2 months with bovine NDT before he saw me). He has obviously been doing some reading the last few weeks, but I'd like to share with him 1 or 2 academic papers that support treating *symptoms*, not lab ranges (or not trying to mimic the output of a healthy thyroid, in a sick one. Can you think of one or two excellent papers that I can download and fax him to help move him along?
I was going to share two JE Midgley papers with him about poor T4 to T3 converters, but was told (above) that no longer applies to me because I am already taking T3 medication 🤷. I thought it could support the reason for adding more T3 to treat ongoing symptoms. Any suggestions? He will read a paper or two by Thursday when we meet again to discuss my new labs, if I fax it to him by Monday.
Thanks for your help and encouragement! And support!
I think your question has just highlighted the quintessential problem with research and treatment for thyroid issues. It is crazy to try and mimic blood results of a ‘healthy person’ with a fully functioning thyroid and aligned H-P-T axis. Once the thyroid is shot (or in some cases gone) the new ‘optimal’ has to be found.
What you need in order to feel well is aligning the tests to YOUR ‘sweet spot’ guided by symptoms and not the converse, a ‘laboratory’ sweet spot to be aligned to.
This is where a departure from their normal practice is required. I’m pretty sure there is not that much out there but I have seen posts from diogenes in the last few months that ACTUALLY mentioned quality of life! 😱😂
In spite of the fact that the T4 to T3 conversion cannot be applied to me, because I have been taking medications with T3 from the beginning, I still think it factors in. I'd be curious what you think.
Six weeks ago, after 6 weeks on a stable dose of bovine NDT, my TSH was 3.47 (1.32-5.04) and my fT4 was 14.0 (10.6-19.7). There was no fT3 test done that time, but the results seems to indicate to me that my TSH was still far from acceptable (2.00-2.50) with a fT4 in the middle of the reference range! That seems to indicate to me, that I am a poor T4 to T3 converter, no?
In the JE Midgley et al paper from 2015 (Variation in biochemical response to l-thyroxine therapy and relationship to peripheral thyroid conversion efficiency) indicate that those with the lowest thyroid volume have the poorest conversion. Given my thyroid surgery 30 years ago to remove a benign tumor, and the subsequent trauma and atrophy of the thyroid, this makes sense as to the reason I am hypothyroid, with negative TPO antibodies. The Midgley et al paper found that poor converters had higher serum fT4 status, which paradoxically to a worsened fT3 level. The fact that my fT4 was right in the middle of the range, but I still had so many physical signs and symptoms of myxedema seems to indicate that I am probably a poor converter. ie the only (or main) therapeutic benefit from the NDT was from the T3 contained in it, not the T4.
If this is true, than the main therapeutic benefit I am currently getting is from the 10mcg of Cytomel (T3) and not the 75 mcg of Synthroid (T4). Does this make sense to you (and others)?
If so, then sending the 2015 Midgley et al paper to my doctor may be helpful.
The other Midgley et al paper I was going to send him was the 2019 one titled Time for a reassessment of the treatment of hypothyroidism, where it talks about the interrelationship between TSH, fT4 and fT3 being highly individual, and the need for a person centred approach (not a lab centred one)
Thoughts?
PS I am open to others, in addition to Charlie-Farley replying to these questions.
your may find these useful as a quick visual aid to support the logic of 'treating to individual needs' .
The main point for any doctor to understand about getting optimal thyroid hormone levels in their patient is 'individuality' ... amongst healthy populations there is a significant individual variation in where their 'normal' levels of T4 / T3 (&TSH) lie. See the 2 following images of data from healthy individuals .
Since healthy individuals are so very different ... why wouldn't individuals taking replacement thyroid hormone also need individual levels of T4 /T3 to function at their best.
If you took subject 8 ('normal' T3 @75% / T4 @50%) and gave them subject 1's 'normal' (T3 @25% / T4 @35%) i imagine they would not feel well .. and vice versa.
(The images are taken from Tania Smiths ThyroidPatientsCanada site, sorry can't remember exactly which of her many articles i pinched them from , but the search facility and index on there is very good ) 2nd image to follow shortly.
Ankrah-Tetteh et al. 2008 'intraindividual variations'
😊👍 I would say it would be her specialist subject on mastermind and she would wipe the floor with her knowledge compared to a certain local surgery! 😂👍
i reckon any opportunity you can use to get any of JEM Midgley's work under a Doctors nose you should take ... 'relevant' or not .... can't remember the in's and outs of the specific ones you mention , but they are all good for discussions about the unreliability of TSH as a dosing tool, and the importance of considering individuality .
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")