I am aware my ferritin is in the lower range and has been going downwards. However when I had full iron panel in August my transferrin saturation was just out of range in the upper level. I have read that one thing that can factor this is dehydration so I am trying to up my water intake. But does anyone know how I can improve my ferritin (and folate) levels - and will it affect my saturation? I currently take Thorne Basic B Complex, magnesium, selenium and vit d
low ferritin high transferrin saturation - Thyroid UK
low ferritin high transferrin saturation
Written by

MrsQ20
To view profiles and participate in discussions please or .
Read more about...
21 Replies
•
SlowDragonAdministrator
Will flag humanbean to hopefully comment
suggest you get full iron panel test including ferritin
Always test early morning, fasting
Thank you - I did full iron panel in August and had recent tests at doctors too so think I have quite up to date information.
MrsQ20,
I think you are getting mixed up with hydration for RBC & haemoglobin results. As these aren’t a part of the T/S% calculation, keeping hydrated won’t directly raise or lower it.
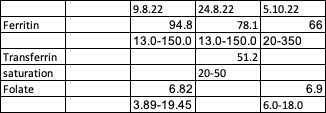
Your T/S% result isn't listed in your graph, just the range 20-50. If you had an iron panel, have you the remaining results and their ranges to share?
Sometimes just posting a photo of your results means important info isn't erroneously left off 😊
radd
I think the Transferrin Saturation is 51.2 and the range is 20 - 50.
MrsQ20
Regarding your folate, it is quite common for people to take a B Complex and still have fairly low levels of folate. I have this issue. I take Thorne Basic B every day, and also a 1000mcg tablet of methylfolate 3 or 4 days a week. I adjust the dose of methylfolate up or down (usually just by one tablet until the next test) each time I get folate tested. I don't know why this problem happens, or why my folate is so variable - but it always happens and I just manage the best way I can.
If I had your results for folate I would want to get it up to a level much closer to top of range.
Is your vitamin B12 level good?
.
Regarding your ferritin... Your result is going down very fast.
9/8/22 - your result was 60% of the way through the range
24/8/22 - your results was 48% of the way through the range
5/10/22 - your result was 14% through the range.
Have you had an accident and lost a lot of blood? Have your periods been horrendously heavy?
When did you start taking the Thorne Basic B, and what dose are you taking?
hb,
Of course! 🤪 Transferrin would always have a much higher range in 200-300mg/dl.
Well done 👏 & thank you 😊
thanks for your reply - I have replied to humanbean
yes sorry for confusion on the transferrin saturation - you are right 51.2 I made it into a table so there was clarity about what has happened since August. I haven't had any accident but I started HRT in May and have had periods since there (not especially heavy). I started on the Thorne Basic B late August and then stopped for a week before recent blood tests. I have taken a methylfolate in the past but not recently. Do you have a product you recommend. I am having a T3 and T4 tested at doctors next Wednesday so can't take any supplements before then. I am a pescatarian and eat fish once or twice a week.
I've read some of your most recent posts, and I can think of a couple of possible reasons why your transferrin saturation is over the range with quickly lowering ferritin.
1) Having had Covid it can disturb all sorts of test results - thyroid hormones and nutrient levels. If this is the cause of your ferritin decreasing it might go back up without any action from you.
2) If you have an MTHFR gene mutation (this is very common - apparently about 50% of the global population has less than ideal genes involving methylation) it can make it difficult for the body to use iron and other minerals.
Some members of the forum have reported that taking methycobalamin (an active form of Vitamin B12) and methylfolate (an active form of folate) that this has had a knock-on effect on improving iron levels. When I refer to "active" B12 and "active" folate" it means that it doesn't have to be converted from a synthetic form of B12 or folate into a form that can be used by the body immediately.
Cyanocobalamin is a common, cheap, synthetic form of B12 that needs to be converted into methylcobalamin to be useful to the body.
Folic acid is a common, cheap, synthetic form of folate that needs to be converted into methylfolate to be useful to the body.
For people with an MTHFR problem this conversion can be slow or difficult or almost impossible.
Some relevant links on B12 and folate :
perniciousanemia.org/b12/fo...
takecareof.com/articles/ben...
chriskresser.com/folate-vs-...
The effect of an MTHFR gene problem is that it slows down or stops the methylation cycle.
And providing the body with "methyl groups" from methylfolate and methylcobalamin will help.
I know that you are taking the Thorne Basic B which already contains the above B12 and folate. You might need methylfolate and methycoablamin in a separate supplement, in addition to the Thorne Basic B, at least for a while, to raise your B12 and folate levels much closer to the top of the range.
If the Thorne product has helped your methylation cycle to start going again, it could be a possible reason for your ferritin to have dropped dramatically, because your body is finally able to make use of your iron.
This is a very old (5 years old) post of mine in which I tried to explain methylation.
healthunlocked.com/thyroidu...
Be aware I'm not a scientist or a doctor and you should take what I say with a healthy dose of scepticism.
Honestly thank you so much - you are always so helpful.
I have read through the links and tried my best to understand. I know the MTHFR gene has been mentioned before. I have found Biocare Nutrisorb liquid formulations of both of these so think I will give that a go alongside the Thorne.
hb,
I haven’t read that old post of yours before. It is really very informative.
I tended to get my info from the old Ben Lynch webpages until he took them down after promoting his book ‘Dirty Genes’ which is very good.
STTM comes into its own now and then. Gonna read all your numerous alternative links now. You have researched this so thoroughly. Great job 😊
")
Sorry Ferratin levels
I have just come across interesting info. It may not be that your ferritin is decreasing although that is what it looks like on paper, it may be that your low B12 was masking your ferritin levels before. When patients are treated with B12, their iron blood count drastically changes.
Check this research article out:
ncbi.nlm.nih.gov/pmc/articl...
I am not saying that is what is going on, but it is possible. So don't panic, over time, perhaps, as both deficiencies are treated, this will "iron" itself out.
You should also take iron every other day rather than every day as this helps your blood serum levels better.
thank you. It does all get confusing! I’m off all supplements this week before blood test. I’m intending to supplement with liquid form methyl folate and methyl cobalamin as well as Thorne basic b once I’ve had blood test. I’m going to see what they does before considering taking iron so I’ll monitor with what you’ve said in mind
They do need each other so I would not recommend not taking iron while you wait to see what your Bs do for you as you could throw yourself even more out of balance and make yourself even more deficient in the meantime. Your thyroid as well as everything else needs iron. Other vitamins need other vitamins and the minerals to be transported to where they need to be and to work.
what is the best form to take it? I’ve taken floradix before but as I’m already taking the Thorne wondered if this is too much of other things?
I get ferrous glucinate 300 mgs from my GP. I take one every other day as research shows this alternate day taking builds serum levels better than taking every day. Other people here may have better suggestions as to supplements though as the NHS usually supply the cheapest. I can tolerate it even though my tummy is not the best and it does not constipate me unlike many other iron supplements.
I know it sometimes feels we take so many supplements we rattle, but iron/ferritin is really not one to cut out, especially if you know you are low already. Just don't take it near other pills and supplements!
Not what you're looking for?
You may also like...
Transferrin Saturation
I have a GP appointment a week Monday. Recently had a Medichecks nutrition test and results:...
Iron, Ferritin, transferrin and transferrin saturation index
Could someone please explain the differences between these and which ones are important to achieve...
Ferritin and transferrin saturation high in range
Hi
I've been working so hard on getting myself well and gave really made so much progress. I've...
Low ferritin, high iron
I recently got a bunch of lab tests done by a functional medicine doctor. I thought I had too much...
low ferritin 32 ,High transferrin 45%
hi
I have high transferrin saturation 45% range bottom 40%
Low ferritin 32 bottom of range is......