can I have some feedback please on my results. I’ve been on liothyronine for 6weeks and don’t feel any different. 75 levothyroxine 5 liothyronine also on aspirin and Bumetimide and multivitamins thank you.
results : can I have some feedback please on my... - Thyroid UK
results
Written by

raine-wager
To view profiles and participate in discussions please or .
Read more about...
13 Replies
•
SeasideSusieRemembering
raine-wager
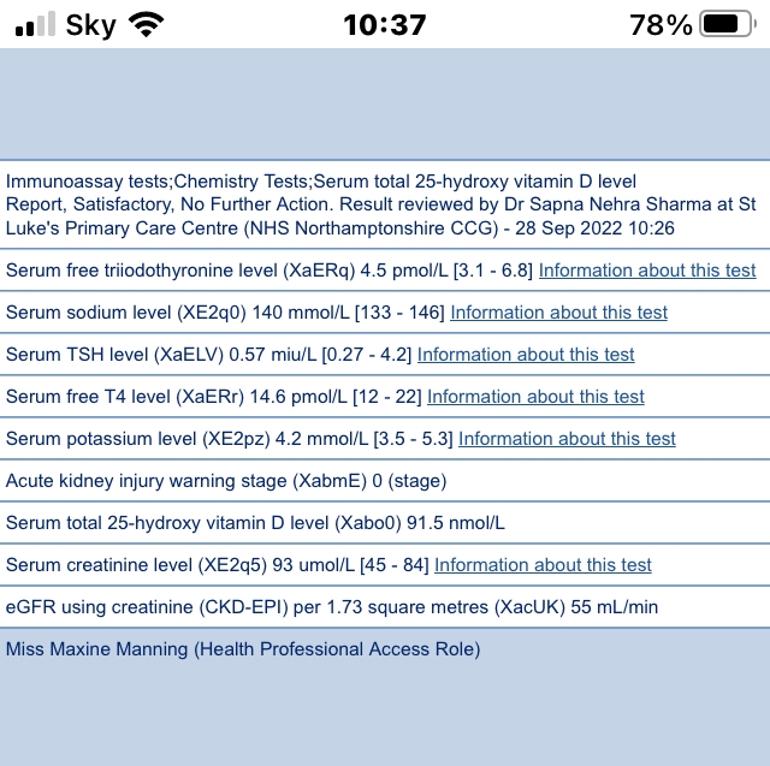
Did you leave the advised time gap between last doses and test, ie last dose of Levo 24 huors before test and last dose of T3 8-12 hours before test?
If so then your FT4 level is very low, it's now only 26% through it's range. What was it before it was reduced by the endo from 100mcg to 75mcg. They all seem to make the same mistake of thinking that Levo needs to be reduced when adding T3, this isn't always the case. If FT4 is over range or at the top of the range then yes, reduce the dose of Levo, but if it's around say 75% through range or less then there is no need because adding T3 reduces FT4 anyway.
I think you need your Levo put back up to 100mcg.
Your FT3 is 37.84% through range which again is low and you will need more T3 added. However, we can't add both at the same time so I'd add more Levo now, wait and retest in 6-8 weeks, then that should increase your FT4 and also increase FT3 to some extent depending on how much natural conversion you have. Then you can see if you need to add more T3, which I think you will. 5mcg T3 is a very low dose.
yes I left the time, go says they are satisfactory 😫 thank you
go says they are satisfactory
Is your GP commenting on your thyroid results or all the results generally?
For the thyroid results then the GP will say satisfactory, they are within range and that's all they care about, they have no notion of "optimal" levels or any symptoms that we may still be experiencing.
However, what have your thyroid results to do with your GP at the moment, it's a trial initiated by your endo so it's your endo who should be commenting and making any dose adjustment. When are you due to consult with your endo again?
I think it’s 6 months from starting liothyronine before I see the consultant again. I have a great nurse who takes my bloods I asked her to do the thyroids test.
Are there no planned increases from 5mcg before you see your endo again?
6 months is a long time to leave between initiating T3 and next consultation, particularly when on such a low dose. Many endos start patients on 20mcg T3 - which is too much, we should increase gradually over time by 5mcg increments to reach that - some endos will only prescribe 10mcg in total, others 20mcg, but 5mcg isn't going to do much. Hopefully at the end of the 6 months, if still on 5mcg, your endo doesn't turn round and say that the trial has failed because you've not improved much and then remove your T3. That would be a very unfair trial.
hi SeasideSusie, can you tell me why adding T3 reduces fT4 levels please, I haven’t come across this before
No, I'm afraid I can't tell you. I don't have any links to any science or articles. But from personal experience and responding to innumerable posts from members I can say that test results show that taking T3 increases FT3 level and reduces FT4 level.
Maybe someone else knows the science, you could make a new post asking about this.
I can only think that taking T3 reduces TSH which in turn suppresses T4 production? My TSH is permanently suppressed so I suppose I don’t produce any.
Perhaps diogenes can help us with that question 😊
The sensitivity of the pituitary to thyroid hormone is roughly equal for T4 and T3. By that I mean that on average this is the case with how euthyroid levels of T4 as FT4 and T3 as FT3 compete in terms of effect. But this equality comes from FT4 being 3 times the FT3 level in blood. Therefore we can safely say that a) normal FT4/FT3 levels show equality of action on the pituitary, but b) since there is only 1/3 the FT3 level compared with FT4, a T3 per molecule has 3 times the effect as a molecule of T4. Now, with this knowledge we can visualise what happens with T3 therapy on FT4 levels in treated hypothyroidism ( in the case of still having some thyroid gland working ). Its T3 production declines much less than T4. Taking T3 will be much more influential in that it will more easily suppress the pituitary than T4. Thus with a partly working thyroid, TSH suppression will lead to reducing both the T4 produced by the thyroid, but also inhibits T4-T3 conversion. Thus the FT4 will steadily rise owing to poorer conversion in the body.
Many thanks for your explanation, I think I understand that 😊 Does the same apply with those of us with no thyroid/working thyroid following RAI ablation?
The phenomenon in this case comes from the different balance of T4 and T3 taken in than that of normality. Usually T3 is taken in at a little greater comparative level to the T4, so the body deiodinases are again inhibited
Thank you😀
Not what you're looking for?
You may also like...
Help with results please
Latest results on 100 Levo and 30 liothyronine.
Tsh <0.01
Ft3 6.9 (3.6-6.3)
Ft4 16 (12-22)
Dr...
Blood test results
My liothyronine has been stopped abruptly by my GP and my consultant has written to my doctor.
In...
test results help
I would love some advice with what to ask my family doctor for medication wise as I am still...
Results Advice
Hi I’m looking to see what you think of my latest bloods please?
I followed all protocols before...
thyroid test results
Hi all, long story short, back in December I was put on a trial treatment of Levothyroxine and...