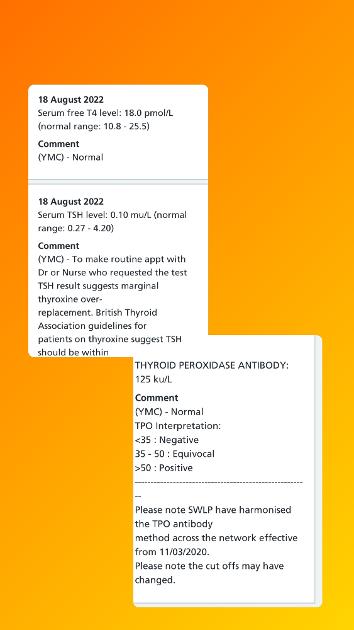
Please could someone help me in interpret the below. First blood test after being diagnosed. Been on 125g levo for 8 weeks. I’m feeling better. Do you think my TSH needs upping and dosage lowering?
I did the blood tests at 8am before I take my meds at 8:30am. Also does the antibodies test mean I don’t have hashimoto's disease?
Thanks so much 🙏🏼
Written by
Racheeeel78
To view profiles and participate in discussions please or .
Do you think my TSH needs upping and dosage lowering?
Your levels could still be settling but absolutely do not lower your dose and this is why:
FT4: 18 (10.8-25.5) = 48.98% through range
The aim of a treated hypo patient on Levo only, generally, is for TSH to be 1 or below with FT4 and FT3 in the upper part of their reference ranges, if that is where you feel well.
Your FT4 is below half way through range so depending on how you feel you might need a dose increase.
Don't let your GP adjust dose by TSH alone, regardless of what the notes above say. TSH is useful for diagnosis but once on thyroid hormone replacement it is of little use other than if it's high it tells us we're undermedicated. TSH is a pituitary hormone not a thyroid hormone, it's the FT4 and FT3 that are the thyroid hormones and tell us our thyroid status.
Also does the antibodies test mean I don’t have hashimoto's disease?
My doctor just rang me and has said to reduced to 100g for 6 weeks. I asked if I could do alternate days of 100/125 and she said she needs a clear reading of where I’m at in 6-8 weeks as I’m newly diagnosed so no.
I’m really worried I’m going to start feeling rubbish again. If I self medicate (I have spare) that will mess up next blood tests results. Any advice please?
You are very early in your thyroid journey so it will be difficult for you to start arguing your case at this point.
At this stage it seems as though you may have to go along with your GP. It doesn't seem very fair based on your results but your next test will very likely show a higher TSH and a lower FT4 and then you can start pleading your case.
First of all, make sure you do your next test as we advise:
* Book the first appointment of the morning, or with private tests at home no later than 9am. This is because TSH is highest early morning and lowers throughout the day.
In fact, 9am is the perfect time, see first graph here, it shows TSH is highest around midnight - 4am (when we can't get a blood draw), then lowers, next high is at 9am then lowers before it starts it's climb again about 9pm:
If we are looking for a diagnosis of hypothyroidism, or looking for an increase in dose or to avoid a reduction then we need TSH to be as high as possible.
* Nothing to eat or drink except water before the test - have your evening meal/supper as normal the night before but delay breakfast on the day of the test and drink water only until after the blood draw. Certain foods may lower TSH, caffeine containing drinks affect TSH.
Last dose of Levo should be 24 hours before blood draw. This avoids measuring hormone levels at their peak after ingestion of hormone replacement. Take your thyroid meds after the blood draw. Taking your dose too close to the blood draw will give false high results, leaving any longer gap will give false low results.
* If you take Biotin or a B Complex containing Biotin (B7), leave this off for 7 days before any blood test. This is because if Biotin is used in the testing procedure it can give false results (most labs use biotin).
These are patient to patient tips which we don't discuss with phlebotomists or doctors.
When you have got the results from your next test, if your results are higher TSH, lower FT4, and you are symptomatic then list all your symptoms or use this tick list from ThyroidUK to show your GP:
Fine tuning of the dose could be necessary in some patients
* aim of levothyroxine treatment is to make the patient feel better, and the dose should be adjusted to maintain the level of thyroid stimulating hormone within the lower half of the reference range, around 0.4 to 2.5 mU/l. If the patient feels perfectly well with a level in the upper half of the reference range, then adjustment is unnecessary
If TSH is between 2 and 2.5 use this and the one below :
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
Also, Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He confirmed, during a talk he gave to The Thyroid Trust in November 2018 that this applies to Free T3 as well as Total T3 and this is when on Levo only. You can hear this at 1 hour 19 mins to 1 hour 21 minutes in this video of that talk youtu.be/HYhYAVyKzhw
You can obtain a copy of the article which contains this quote from ThyroidUK
Email : tukadmin@thyroiduk.org
and ask for the Dr Toft article from Pulse magazine. Print it and highlight Question 6 to show your GP.
The recommendations in this guideline represent the view of NICE, arrived at after careful consideration of the evidence available. When exercising their judgement, professionals and practitioners are expected to take this guideline fully into account, alongside the individual needs, preferences and values of their patients or the people using their service. It is not mandatory to apply the recommendations, and the guideline does not override the responsibility to make decisions appropriate to the circumstances of the individual, in consultation with them and their families and carers or guardian.
In other words the GP should take into consideration your symptoms and not stick blindly to guidelines.
Thank you so much for all this information. I think dr is being precautions of me going over active as I lost my mother to heart attack - she was just 45.
Annoying I feel great on the 125g- the only notable symptom was my eyes have felt a little bulgy in the mornings. I did do all of the below in regard to fasting and having bloods in the morning on this blood test.
I will save all the info below for my next blood results. My doctor is good on the whole and has referred me to a weight loss clinic to help with the weight gain (2 stone) as I’m hoping to try for ivf soon.
With having Hashimotos should I avoid gluten & dairy? I’m not a celiac.
I do have private health through work- would you recommend going private so can get my t3 tested. NHS will not prescribe t3. Or would you wait until next blood results so not overriding GP so early on?
Will my FT4 definitely lower with the 25g decrease in levo or could it still continue to rise. I’m just worried I’ll feel progressively worse now?
I did keto diet for over a year pre-pandemic and Felt great- maybe something to consider? I only started eating carbs again due to lockdown.
would you recommend going private so can get my t3 tested. NHS will not prescribe t3. Or would you wait until next blood results so not overriding GP so early on?
I personally wouldn't do anything about seeing a private doctor, not at the moment anyway, give it a go with your GP, we have lots of evidence, experience and information we can pass on to you to help you on your way, and if you go private it might just mean that your GP will expect you to continue your thyroid care with your private doctor and no longer prescribe on the NHS.
You don't need to see a private doctor for the FT3 test. Cheapest way is to use an NHS lab at Exeter hospital who offer the basic thyroid panel as a fingerprick test to the general public for £26.10 using code here:
There are other private labs but if you use that one (if the basic test is all that you want) it will be difficult for your GP to dismiss the results because it's an NHS lab whereas any other private lab they could quite easily not accept.
I would wait until you've done your next test with your GP, it's early in your journey so you need to give it a go for now.
Will my FT4 definitely lower with the 25g decrease in levo or could it still continue to rise. I’m just worried I’ll feel progressively worse now?
Thank you so much, I’ll stick with my GP and see where I’m at in 6 weeks when I have next bloods. If I feel terrible I will make an appointment and explain that to GP between now & then.
I’ll do that thyroid test using the link you gave- thank you! Would you recommend doing that in 6 weeks too so my doctor will have those results after 6 weeks on the lower dose- so I don’t get told the results were when my TSH was out of range?
Would you recommend doing that in 6 weeks too so my doctor will have those results after 6 weeks on the lower dose
You should wait 6-8 weeks after any dose change for levels to settle before testing (I find I'm still feeling a difference at 8-10 weeks), so really you would have to do the private test at 5 weeks to have the results back for when your GP test comes back. I think that is too soon.
I think what I would do is let the GP do their test, see what the results are. If you're lucky there will be TSH and FT4, unlikely to be FT3. So if your results show that you need an increase and your GP is unwilling to raise your Levo back to 125mcg, you can say that you have spoken to ThyroidUK which is the thyroid charity recommended by the NHS for information about thyroid disease (use the word spoken and don't mention internet or forums) and they have advised to have a full thyroid panel which includes FT3 because it's FT3 which is the most important test.
[T4 is a pro hormone, a storage hormone that has to convert to T3 which is the active hormone which every cell in our bodies need. Testing FT4 and FT3 shows our thyroid status, just testing TSH and FT4 can't show how much of the active hormone T3 that is available for our cells to use.]
You can then ask if she can get TSH, FT4 and FT3 tested all at the same time, it's unlikely that she can because even if she requests it it's the lab that makes the decision as to whether it's tested and if TSH is in range they're unlikely to test FT3. So then you can say that you know that NHS Exeter hospital offers this test to the general public so you are going to get that test done and will bring the results to show her.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.