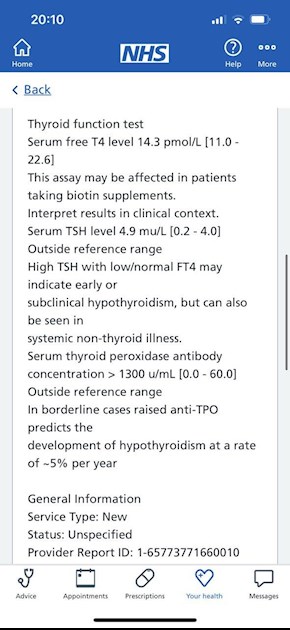
hi im new to his forum im really worried as i have searched up blood test results from last year and is it indicating haishmoto ? i still have trouble losing weight and tired all the time, they put me on 100mcg levo last year and never tested the antibodies again thank for anyone that can help me
please help with results do i have hashimoto di... - Thyroid UK
please help with results do i have hashimoto disease ?
Written by

ali2341
To view profiles and participate in discussions please or .
Read more about...
18 Replies
•
oh and just to add my tsh is 2,2 now with the 100mcg levo but still find it hard to lose weight and tiredness,
Hi ali2341, welcome to the forum.
You still can't lose weight because you are under-medicated. Your TSH is still too high. It should come down to 1 or under. You should have been retested after six weeks and your dose increased by 25 mcg.
Yes, you do have Hashi's, which has caused your hypothyroidism. No point in retesting antibodies after the first positive results, because antibodies fluctuate, but Hashi's doesn't go away.
What is it you're worried about? ")
i feel like crap on levo, im thinking to get some t3, or maybe you might be right to increase dose, will have to get full panel done privately as my gp is awful.
Until either your TSH is 1 or under or your ft4 is at the top of its range you should stay on levo only. Your 2.2 TSH means you need an inc in dose. This may resolve symptoms.Why is it too soon to start t3? You haven't yet been on a high enough dose of levo to bring TSH down and to have high enough ft4. In a normal person ft4 is on average 50% through range and hypos need it higher so currently your ft4 is too low. This is mirrored in your raised TSH which on levo ideally should be 1 or lower on levo.
You can only tell if you are a poor convertor of t4 to t3 when you are on levo only. Being a poor convertor is justification for getting t3. But to be able to tell if you are a poor convertor TSH has to be down around 1 or under on levo only .
T3 is not a quick or easy fix and it is not freely available or prescribed. It can take years of optimising doses of both levo and t3 until you find a dosing regime that suits. GP surgeries do not test ft3 as a matter of routine so you will need to organise regular blood tests as you alter your doses as when on t3 you must test ft3.
SlowDragonAdministrator
When was last test done
Just testing TSH is inadequate, especially with Hashimoto’s
ALWAYS test thyroid levels early morning, ideally before 9am and last dose levothyroxine 24 hours before test
Request thyroid levels retested including Ft4 and Ft3
Also request vitamin D, folate, ferritin and B12 are tested
Plus coeliac blood test if not been tested yet
in jan this year , vit d was low but they have me tabs for that ,
How low was vitamin D
How much vitamin D are you currently taking
Vitamin D tablets must be four hours away from levothyroxine
Thyroid patients often need higher dose vitamin D than other patients
You must test vitamin D twice year when supplementing
Aiming for at least around 80nmol minimum
NHS easy postal kit vitamin D test £29 via
it was 23.9 nmol/l
So presumably you had loading dose vitamin D That’s 300,000iu in total over 6-8 weeks
Vitamin D levels should be retested at end of prescription
And you should be advised to take an ongoing maintenance dose
Trial and error what dose that is
Some only need 1000-2000iu
Many thyroid patients need higher dose
SlowDragonAdministrator
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested.
Very important to test vitamin D, folate, ferritin and B12 at least once year minimum
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
List of private testing options and money off codes
thyroiduk.org/getting-a-dia...
Medichecks Thyroid plus antibodies and vitamins
medichecks.com/products/adv...
Blue Horizon Thyroid Premium Gold includes antibodies, cortisol and vitamins
bluehorizonbloodtests.co.uk...
If you can get GP to test vitamins and antibodies then cheapest option for just TSH, FT4 and FT3
£29 (via NHS private service ) and 10% off down to £26.10 if go on thyroid uk for code
thyroiduk.org/getting-a-dia...
NHS easy postal kit vitamin D test £29 via
With TSH over 2 you need 25mcg dose increase in levothyroxine
Bloods should be retested 6-8 weeks after
Which brand of levothyroxine are you currently taking
Do you always get same brand levothyroxine at each prescription
Many people find different brands are not interchangeable
TSH should be under 2 as an absolute maximum when on levothyroxine
gponline.com/endocrinology-...
Graph showing median TSH in healthy population is 1-1.5
web.archive.org/web/2004060...
thanks so much for the reply the brand im taking is teva and get it regularly , i been researching it says on net that i should be taking 1.6mcg of levo per kg of weight, im 5 10 and weigh 120kg
Are you lactose intolerant that you are on Teva brand
Teva brand upsets many people
Ever tried a different brand
Print out guidelines on dose by weight
Request 25mcg dose increase in levothyroxine
Bloods should be retested 6-8 weeks after each dose increase
Likely to need further increase in levothyroxine after next test
Meanwhile request coeliac blood test, plus folate, ferritin and B12 levels tested
nope not lactose intolerant, is this brand not good ?
Approx 60-70% of Hashimoto’s patients are lactose intolerant
Have you only ever had Teva brand
Many people find Levothyroxine brands are not interchangeable.
Many patients do NOT get on well with Teva brand of Levothyroxine.
Teva contains mannitol as a filler, which seems to be possible cause of problems. Mannitol can change gut biome
Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
But for some people (usually if lactose intolerant, Teva is by far the best option)
Teva, Glenmark or Aristo (100mcg only) are the only lactose free tablets
Most easily available (and often most easily tolerated) are Mercury Pharma or Accord
Mercury Pharma make 25mcg, 50mcg and 100mcg tablets
Accord only make 50mcg and 100mcg tablets
Accord is also boxed as Almus via Boots, and Northstar 50mcg and 100mcg via Lloyds ....but Accord doesn’t make 25mcg tablets
beware 25mcg Northstar is Teva
List of different brands available in U.K.
thyroiduk.org/if-you-are-hy...
Posts that mention Teva
healthunlocked.com/search/p...
Teva poll
healthunlocked.com/thyroidu...
Once you find a brand that suits you, best to make sure to only get that one at each prescription.
Watch out for brand change when dose is increased or at repeat prescription.
New guidelines for GP if you find it difficult/impossible to change brands
gov.uk/drug-safety-update/l...
If a patient reports persistent symptoms when switching between different levothyroxine tablet formulations, consider consistently prescribing a specific product known to be well tolerated by the patient.
academic.oup.com/jcem/artic...
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
Levothyroxine is an extremely fussy hormone and should always be taken on an empty stomach and then nothing apart from water for at least an hour after
Many people take Levothyroxine soon after waking, but it may be more convenient and perhaps more effective taken at bedtime
verywellhealth.com/best-tim...
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap.
Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
(Time gap doesn't apply to Vitamin D mouth spray)
If you normally take levothyroxine at bedtime/in night ...adjust timings as follows prior to blood test
If testing Monday morning, delay Saturday evening dose levothyroxine until Sunday morning. Delay Sunday evening dose levothyroxine until after blood test on Monday morning. Take Monday evening dose levothyroxine as per normal
REMEMBER.....very important....stop taking any supplements that contain biotin a week before ALL BLOOD TESTS as biotin can falsely affect test results - eg vitamin B complex
hi thankfully im not lactose intolerant, i drink milk and eat cheese everyday with no problems, just wanted to ask are the finger prick medichecks blood tests accurate or is it better to do normal vein test ? also just wanted to add i was taking vit d tablets from doctors , i have took them in past years ago but i had to stop this time as i was getting huge painful nodules lumps on my skin around thighs and sides of head so i had to stop this year ,sorry for so many questions but thanks for the help i really appreciate it
SlowDragonAdministrator
pathlabs.rlbuht.nhs.uk/tft_...
Guidelines on Treatment with Thyroxine:
In the majority of patients 50-100 μg thyroxine can be used as the starting dose. Alterations in dose are achieved by using 25-50 μg increments and adequacy of the new dose can be confirmed by repeat measurement of TSH after 2-3 months.
The majority of patients will be clinically euthyroid with a ‘normal’ TSH and having thyroxine replacement in the range 75-150 μg/day (1.6ug/Kg on average).
The recommended approach is to titrate thyroxine therapy against the TSH concentration whilst assessing clinical well-being. The target is a serum TSH within the reference range.
……The primary target of thyroxine replacement therapy is to make the patient feel well and to achieve a serum TSH that is within the reference range. The corresponding FT4 will be within or slightly above its reference range.
The minimum period to achieve stable concentrations after a change in dose of thyroxine is two months and thyroid function tests should not normally be requested before this period has elapsed.
yes this is what im seeing on net, my weight is 121 kg, and im only on 100mcg, i will do another thyroid blood test next week hopefully and then will request to be put on higher dose of levo. thanks for help
Not what you're looking for?
You may also like...
Do I have Hashimoto's? and latest results.
I never really understood it and asked my docs recently if I have hashimoto's and...
Do I have Hashimoto?
and would be really grateful for some guidance.
I was put on levothroxine about 10 years ago when...
Normal TSH but all the symptoms of Hypothyroidism and I have Hashimoto disease. Help!
keep checking. For the last 2 years I’m very tired all the time, can’t loose weight (I run 3x a...
Do I have Hashimoto's?
hypothyroid state. I had antibodies tests and my results are:
Thyroglobulin Antibody <10 (<...
Do I have Hashimoto's?
Hi,
My recent blood test results for thyroid are as follows:
TSH - 6.25
FT4 - 12.4
FT3 - 3.8
TPO Ab...