In August 2021 I was put on a "trial" of Levothyroxine by my GP after me having quite the battle to get prescribed. Over 4 yes post hysterectomy I'd went out of range and barely back in range if at all, several times.
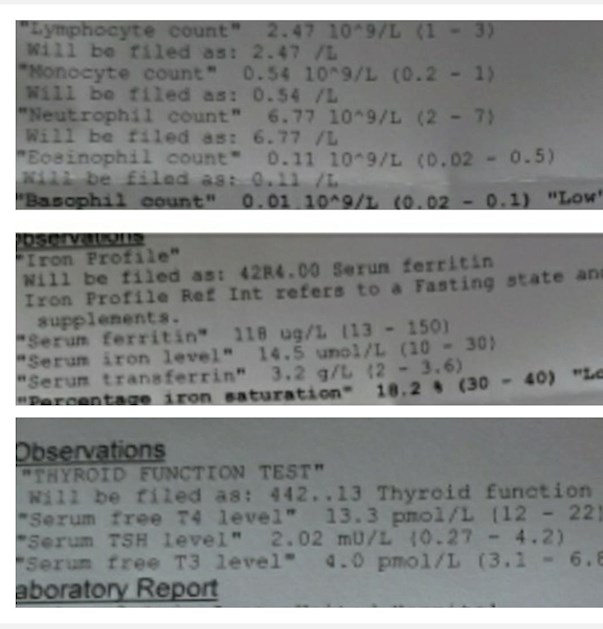
On the results that follow my TSH doesn't seem to have raised on 25mg levo. I barely came back in range too on Free T4 at 13.3 (12-22) range.
A query I have is my ferritin dropped 61 points in 3 months , from 179 to 118 so high to in range, yet the "iron saturation " is Low? I don't understand this part.
I intend to ask the GP tomorrow to increase my Levothyroxine dose.
There is also 1 x low reading in the white blood cell sub categories?
Any advise greatly received.
Thank you in advance
K.
Written by
BetterDayzAhead
To view profiles and participate in discussions please or .
You are not looking to raise your TSH. On the correct dose of levo your TSH should reduce to below 2 and probably around 1.Your ft4 and ft3 need to rise as these are the thyroid hormones and most need them at least halfway through the ranges. There is no set figure to aim for though, it is where you feel well .
You need next 25mcg dose increase in levothyroxine
Bloods should be retested 6-8 weeks after each dose increase
Likely to need further increase in levothyroxine after next test
You have high thyroid antibodies, confirming autoimmune thyroid disease also called Hashimoto’s
ESSENTIAL to test vitamin D, folate, ferritin and B12 at least once a year
Request GP test vitamin D and folate and B12
Are you still on folic acid supplements for low folate?
On levothyroxine the aim is to increase the dose slowly upwards in 25mcg steps until Ft3 is at least 50% through range and on, just levothyroxine Ft4 likely to need to be at least 70% through range
Thank you, do I have a reading for high thyroid antibodies I don't see that on my results SlowDragon ? I will go fetch newest blood results today they are printed out for me. I will definitely push for next 25mg increase. I've been getting Mercury Pharma, Workhardt and TEVA brands and the Pharmacist will only keep giving me what they have available as I'm in N. IRELAND and greatly affected by supply chain limitations after Brexit. Thank you so much.
If a patient reports persistent symptoms when switching between different levothyroxine tablet formulations, consider consistently prescribing a specific product known to be well tolerated by the patient. If symptoms or poor control of thyroid function persist (despite adhering to a specific product), consider prescribing levothyroxine in an oral solution formulation.
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
Levothyroxine is an extremely fussy hormone and should always be taken on an empty stomach and then nothing apart from water for at least an hour after
Many people take Levothyroxine soon after waking, but it may be more convenient and perhaps more effective taken at bedtime
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap.
Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
(Time gap doesn't apply to Vitamin D mouth spray)
If you normally take levothyroxine at bedtime/in night ...adjust timings as follows prior to blood test
If testing Monday morning, delay Saturday evening dose levothyroxine until Sunday morning. Delay Sunday evening dose levothyroxine until after blood test on Monday morning. Take Monday evening dose levothyroxine as per normal
Many patients do NOT get on well with Teva brand of Levothyroxine.
Teva contains mannitol as a filler, which seems to be possible cause of problems. Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
But for some people (usually if lactose intolerant, Teva is by far the best option)
Teva, or Aristo (100mcg only) are the only lactose free tablets
Yes always on empty and 9am appointment. No biotin supplements or any for that matter...thank you, Il post up new printed results later today. Il fetch them from GP ~ thank you as always for your helpful advice.
Its awful to state but GPs fought me hard on this for 3 years going on 3. They don't understand bottom ranging, they see it as in range and very vhelmently fight a prescription. I probed her interest in increasing me 3 weeks ago so she's waiting on my new bloods yhat I will likely have to highlight to her as will be barely in range! Sorry to say but they don't seem to care if you say you are exhausted, rock bottom, Struggling at home. I brought my husband in for support last time so she wd be on her best behaviour with me. "We will look at your blood results" this has been going on to my knowledge since Inwas being tested for this st 10yrs old, yet only in the last few years have I joined this group and know I need an optimum range for me, not to be bottom ranging. I know now to get print outs and assess my own results, for years I took their deduction on in range and hence I've been an exhausted sleepy child/adolescent/adult all my days.
I just wish GP wouldn't fight as much with her stead fast belief that in range is OK! ~ Thank you.
It's almost as if they have been indoctrinated (!) and led to believe that numbers are the only diagnostic guide and that computers can "read" the patient. Rubbish! That needs good old fashioned clinical evaluation.....signs and symptoms.They overlook the fact that we are humans, not machines, and therefore all different with different needs.
It took decades to discover what was wrong with my thyroid function... and that was thanks to support from here. Medics were clueless.
Try showing her the paper I linked above....authors are renowned thyroid scientists including TUK's diogenes
And this article by Paul Robinson includes references to scientific papers
No ranges given and missing values. I'm just disgusted with this, my Sister got out of work to collect this and its not complete, no T3 T4 and no diabetes data.
New bloods from 15th March. They have literally printed out with no ranges !
Email Thyroid U.K. for list of recommended thyroid specialist endocrinologist and doctors
There may be some on list in NI
tukadmin@thyroiduk.org
GP’s should follow clear guidelines to SLOWLY Increase dose levothyroxine upwards until on, or near full replacement dose
Levothyroxine doesn’t top up failing thyroid, it replaces it (a fact many GP’s just don’t grasp )
Use guidelines on dose levothyroxine by weight to argue/push for each dose increase in levothyroxine ……
Even if we frequently don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or near full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
Well, the ranges for thyroid testing seem to me to be the problem. The GPs mainly don't have the training to help us and are guided by the ranges given. Surely those should change. I wonder who sets them?
It's not the ranges per se that are the main problem but the ability of medics to interpret the lab results.The labs should ideally be used in conjunction with the signs and symptoms presented by the patient!
I agree but in reality my previous GP wasn't helpful re symptoms. When I asked for a 25mg increase he said "Over my dead body"! I wore him down and next time saw a different GP and continued on that dose.
How does he think thyroid disease was diagnosed before tests were developed!
Clinical evaluation....signs and symptoms
And these are personal to each patient.
He is treating numbers, not the patient.
Have you had a full thyroid test or is your doctor convinced( wrongly) that TSH is the bees knees!!TSH, FT4, FT3, vit D, vit B12, folate, ferritin and antibodies TG and TPO
It sounds as if you may possibly....
have been undermedicated for some time
have low essential nutrients levels ( above)
have poor T4 to T3 conversion
not respond well to levo
benefit from adding some T3...
A GP who responds with " over my dead body" is a disgrace
Can you see another GP who has more empathy with his patients...and hopefully a better understanding of thyroid disease?
He always was an awkward disgrace. We moved to another town and have been with a new surgery for 2 yrs. I've only spoken to the GP via phone consultations due to lockdown of course. This one seems more amicable but I will need to help him along by asking for the specific testing. I think he will stutter a bit and I'm prepared for him to say Lab won't do those. If so I'm going to ask him to do a private test, don't think he can refuse that one. I'm due for retesting (8 weeks) at the end of April. I'm taking 75mg, having changed to Mercury Pharma from Teva. Last time I took 100mg the T4 was 28, TSH 0.02.... I also felt very unwell. Maybe I need to try adding 1/2 a tablet? I do think I need more levo. Maybe change to Eltroxin? The other option is a referral to an endo.
Thanks so much. Currently overweight by 3 stone (medically/surgically injured during hysterectomy so mobility is affected) so that's me 90kilos x 1.6mg is 144 so 150mg and current sat on 25mg tablet! Ive Put up the results print out from todays trip to GP (my sister got out of work to go) on the thread and its 1 sheet and must be wrong, like a summary? no ranges and values missing for T3 T4 Ferritin and their full count must include a vitamin D....I'm fed up to the back teeth with this GP's Surgery. I've emailed and asked for a print out with lab ranges. Thank you SD
25mcg has probably made you feel worse. At least if that is the case, it might also make your numbers look worse! It's enough for your pituitary to relax and stop sending out hormone to instruct your own thyroid to produce hormone. But it's not enough to take over. You could well be getting less thyroid hormone now than before you started. They really are clueless. So many GPs are clueless about this.
SD, after a lengthy talk with a Locum today, she's placing me on an additional 25mg only at weekends!!!! This conversation was going on so long I had accepted I wasn't getting an increase. I actually said I respect you are bound by guidelines but do you treat the TSH level or the patient? I am having multiple symptoms which had stabilised on 25mg in the early days, its been a slow return to the full list of symptoms I had prior to the 25mg of Levothyroxine. I want to speak with Dr Young the male who did say to me one we must treat the patient...so deflared today, conversation drained the life of me and I have a banging headache as usual.
Thank you SD. Shes actually havingva chat with the other GP, I said I'd speak with her if she's not comfortable going outside her TSH level on guidelines. I've explained its not budging too in 3 years, a TSH of 2.2 or 2.4 my optimum level isn't 13.3 T4, because I'm exhausted, having terrible nitemares, acid reflux headache, sensitive to daylight, tinnitus. The whole practice it seems behave like this though I will try Male GP who did say before to treat the patient not the print out!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.