Some background is that I was stable on 200mcg for about 10 years until I had my child around 6.5 years ago. Since then it’s not been at all stable and I have gone down and down in levothyroxine. I always use the same brand (Eltroxin). I’m now down to 125mcg but have only been in that since 14 Jan 22. Before that for a few months I was on 150mcg one day and 125mcg the next. I decided to go down to 125mcg because I have been having problems with my voice. I can’t describe it other than it goes funny and become a real effort to speak.
Please can someone help me to know what’s going on. Could it be a conversion problem? Or is it something else?
Thank you very much.
Written by
AppleOrchard
To view profiles and participate in discussions please or .
You certainly DO have a conversion problem - free T4 is over-range but free T3 is only 29.7% through range. Can you see an endo about a trial of lio (and small reduction in levo)? Are your key nutrients good? Then you can see if, when you eliminate conversion problems, the voice problem disappears, or if this is something else again ... Or it may be quicker to see an ENT person as well, as soon as - but I wouldn't ignore the conversion issue x
That’s a very good idea about checking everything and seeing an ENT. I will call the doctor and see. Although by reducing the levo to 125mcg, it does seem to be a bit better - except when I get very tired. Before reducing, it was there most of the time. It always used to be only there when I was very tired. Thank you very much for your reply.
It´s so sad to see that the lab only recommends the TSH to determine if your dose is appropriate, whether you take levo only or T3+T4.Your FT3 levels are low given your slightly out-of-range FT4 which is indicative of poor T4 to T3 conversion. Nutritional deficiences can affect T4 to T3 conversion: low ferritin/iron, zinc, vitamin B12 and vitamin D just to mention a few. Have you had them tested recently? Sometimes, conversion can improve if all deficiencies are corrected, but it is also likely that you need to add T3 to T4. If on T3+T4, it´s likely your free T4 levels and TSH will drop. Many doctors including endocrinologists are uncomfortable with that. So, unless your current doctor is very open-minded and not obsessed with the TSH, I´d recommend finding a more knowledgeable doctor if you want to try T3.
Thank you very much for your reply. I did have other tests at the time but I didn’t get the results. I will call on Monday to get the rest of the results. Apparently they were all normal. He didn’t redo my vitamin D because he said that between October and now they would only have gone down. (I had them done in October. I will check what it was then but from what I can remember, it was around 74. I may be remembering incorrectly! Sadly most doctors are obsessed with TSH. And they don’t usually do T3. I managed to persuade him to write it on. My TSH is already suppressed. When I used to see Dr Toft he was fine with that.
Unfortunately, "normal" to many doctors just means "anywhere in range", so your levels may very well be suboptimal without your doctor reacting. Most doctors don´t know how to interpret lab results so think that anything within range is fine. When you get your results, post them here (with ranges) for members to comment!You need to have your vit D levels measured again as well. Would it be possible for you to have them tested again?
Yes, that’s certainly true. A GP just has to see everything in range. To my GPs credit she is letting me manage it myself because essentially I know more than her. But I don’t know nearly as much as people on here!
I can ask about having the vitamin D done again. A different GP to my usual said there was no point in getting my vitamin D done again because it will be low. He said that in the winter months it goes low. The time before last it was 54. I think that was in April 21. He said that between April and October vitamin D goes up before going down again in the winter.
Does T3 help the other vitamins and minerals be more within range, as in at the prime levels for functioning well? I hope you understand what I mean. Since Covid, I’m having a lot more trouble explaining myself than I did before. Hopefully it’s short term!
I have not heard of T3 helping vitamins to remain in range, but I hope someone who knows more about that will reply to that question.Do you take a vitamin D supplement? More clued-up doctors like functional/integrative doctors recommend vit D be taken every day. If your doctor knows that your vit D levels are low, they should be tested and any deficiency corrected. It used to be believed that we could only be vit D deficient during the winter months, but some doctors now recommend daily vit D supplements. One doctor once told me that we will store vit D from the sunlight during the summer months and that stored vit D will then provide us with enough vit D to get through the winter months. For a long time, I believed that as I assumed doctors know what they are talking about. When I had my vit D levels checked, it turned out I was deficient. I need a daily vit D supplement to keep my levels in the optimal range.
Again it’s the usual story with a GP - if you’re in range, even only just, you’re fine. So I’m fine, according to the doctor.
I will ask to have them done again by my usual GP and see what she says. She may or may not agree.
When I first started with my thyroid condition 18 years ago, it was only discovered by a registrar who was very keen. I’d had a sore throat for months, plus I pointed to my thyroid and said I’m sore here. I didn’t know it was my thyroid at the time. He dismissed it. But luckily when I went back I saw the registrar. He gave me antibiotics and lots of blood tests. My thyroid results weren’t good but only just out of range.
I will post the results on here when I get them. It’s not so easy in this new medical centre since we moved area almost a year ago.
Does T3 help the other vitamins and minerals be more within range, as in at the prime levels for functioning well?
Could be, yes, indirectly. The reason your nutrients are low is probably because your stomach acid is low, so you have problems digesting food and absorbing nutrients. Your stomach acid is low because your T3 is low - i.e. you are hypo.
Raise the FT3 level and the stomach acid level should rise and your digestion and absorption improve. Well, that's the theory, anyway. Whether or not it will work in practice is another matter. Probably depends on how long you were hypo before diagnosis, and other such variables. You can only try it and see.
Thank you very much for your reply. I find this whole thing very interesting and the replies are so enlightening. I suspect I was hypo for quite some time before being diagnosed. It was definitely at least six months, but I’d say probably a few years.
I look forward to getting my results tomorrow so that I can post them. Apparently they are all normal. The only thing that was out of range is my thyroid. We will see how normal they are once I have them.
Yes, just being 'in-range' does not make them 'normal'. But doctors really do not understand how to interpret blood test results. That's just one of the things they don't learn in med school!
Sorry, I don't have any articles on that particular subject. But, if you look on my profile, you will find many articles about individual nutrients and supplements, like magnesium and calcium, etc.
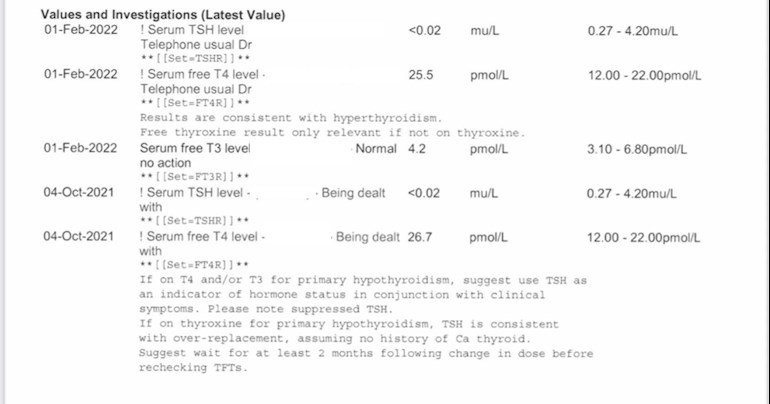
Yes there is a conversion issue which has resulted in a high T4 and a low T3 and also a low TSH :
Sadly in primary care the TSH is deemed the result to track and monitor and since you are now below the TSH range a T4 test is run which shows you over the range and the knee jerk reaction is to reduce your T4 :
What isn't looked at or considered is that your T3 is barely in the range at just under 30% :
T3 is the active hormone and what the body needs at a good % to function and run the body well and currently your running on too low a level of T3 to function.
Too low a level of T3 for you and you will have symptoms of hypothyroidism just as too high a level of T3 for you and you may have " hyper type " symptoms .
Your T3 is said to be " normal " as it is in the range but is it where in the T3 range you need it to be, to be well, and be metabolising your nutrients to keep you well, as that's the most important number to know and maintain.
T4 is inert and a storage hormone and needs to be converted by your body into T3 the active hormone that runs the body which is said to be around 4 times more powerful than T4 with the average person needing to find / convert around 50 T3 daily just to function.
You ability to convert T4 into T3 can be compromised by low levels of ferritin, folate, B12 and vitamin D and also consider that inflammation, and any physiological stress ( emotional or physical ) depression, dieting and ageing will also compound conversion.
So - the accepted conversion ratio when on T4 only is said to be 1 / 3.50 - 4.50 - T3/T4 :with most people feeling at their best when they come in at around 4 or under:
So - to find your conversion ratio you simply need to divide your T3 into your T4 and I'm getting yours coming in at 6.07 showing your conversion very poor and wide of centre.
You say you were well on a much higher dose of T4 - do have these results, out of interest ?
You were obviously metabolising at this higher dose and the T4 was converting to a high T3 which is what we all need, and not, not converting and showing as an over range T4.
I would think your metabolism has nose dived with these successive decreases in T4 which leaves you now with an over range T4 as you are not on enough T4 to metabolise and convert the T4 into T3 .
Likely your ferritin, folate, B12 and vitamin D have also taken a tumble as when you're not metabolising you will have trouble extracting essential nutrients from your food to maintain your core strength strong and solid.
Thank you so very much for your very detailed reply. It’s unbelievably helpful.
Somewhere I do have all my previous results. I will look them up.
A few years ago Dr Toft suggested adding in T3 but somehow it didn’t happen. I am not sure why.
I have also been struggling with weight. I am not eating much more than I used to, although I have put on about 3kg. (I have lost 2kg of those kilos in the last two weeks because of Covid.)
I will get the rest of my results tomorrow when I call the GP.
It’s interesting you say that the main driving force with thyroid is the T3 and yet T3 isn’t systematically checked. And you can’t get T3 on the NHS. It’s truly shocking.
I wish I was still under Dr Toft. He was such an amazing doctor. He wasn’t guidelines or numbers led. He knew his stuff when it came to thyroid like no one else I ever came into contact with.
Thank you very much again. I now need to think about where I can get some T3 from. UK prices are outrageous.
I’m very grateful to you for taking the time to reply.
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water and last dose levothyroxine 24 hours before test
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
Personally I'd ensure my ferritin, folate, B12 and vitamin D were up and maintained at optimal levels as no thyroid hormone replacement works well unless your core strength is strong and solid.
I think it's interesting that you were well and metabolising on a larger dose of T4 than that currently prescribed and believe you have been dosed and monitored on your TSH which unfortunately is totally misleading and has ultimately left you unwell and asking questions.
You may find some endo's will be reluctant to prescribe T3 when the TSH is already low suppressed.
The TSH was originally introduced as a diagnostic tool to help confirm a diagnosis of hypothyroidism.
The TSH was never intended to be used once the patient was on any form of thyroid hormone replacement as then you need to be checking that the T3 and T4 are balanced in the ranges, at around a 1/4 ratio T3 / T4, and high enough in the ranges to be acceptable to the patient.
I will check the levels tomorrow. What would you say optimal levels are for each? If I didn’t get my D done, I’m going to ask for it. Then hopefully I’ll have all the tests I need, except the thyroid antibodies. I will probably need to have it done privately.
I was well on 200mcg for a long time. It was Dr Toft who monitored me. He told me that a suppressed TSH was fine as long as T3 was okay. I’m going to see if I have old blood tests and see if my T3 has always been low. I think it has. It’s always been 4 something.
I watched Dr Toft’s video the other day and he talked about the origins of testing and that’s when all the patient complaints began. It was fascinating.
I wonder about being given T3 when my TSH is already suppressed. I guess I’ll have to see what happens.
Well your original post on here states your T3 was top of the range ;
I also read you were under Professor Toft for some 15 years and came on here looking for recommendations of whom you should see, on his retirement.
So, I presume your cause of hypothyroidism too complex for treatment in primary care and do you remember what was your original diagnosis ?
Maybe your TSH has never been a true reflection of what's going on.
My TSH is stuck down as I have Graves Disease and am post RAI thyroid ablation.
Being dosed on only a TSH yearly blood test in primary care left me very unwell and
I was refused a trial of T3 as my TSH was stuck down at 0.01 though my T3 was at just 25% through the range :
I now self medicate with Natural Desiccated Thyroid and Prof Toft's article published in his retirement year from the NHS instrumental in my learning curve - though it fell on deaf ears in the NHS.
I had forgotten that my T3 was quite high but I’m now wondering how high it actually was. Through the NHS app, I’m hoping that all my blood tests will be on there - at least a few years worth and then I can check. I kept a lot but we moved about a bit so my records aren’t in as good shape as they were.
Originally I went to see Dr Toft because the GP didn’t feel confident increasing my medication. Dr Toft ran various tests and said I didn’t have Hashimoto.
It’s awful that you weren’t able to trial because you’re TSH was stuck down. I hope you managed to work out the correct dose for yourself. Do you think NDT is better than T3/4 medication? How did you know what dose to give yourself?
My TSH is stuck too. If my TSH was more normal, I would feel even worse than I already do.
Most of what Dr Toft said latterly fell on deaf ears within the NHS. It’s very sad because he spoke more sense than anyone else in the field.
The TSH doesn't cause symptoms - it's simply a signal from the pituitary to stimulate the thyroid and if you've a problem with your pituitary you'll have trouble being dosed to wellness in primary care as the knowledge and skill set isn't there.
Fighting the NHS simply exacerbated my symptoms so I resorted to self medication.
Without a thyroid it's likely one needs full spectrum thyroid hormone replacement.
I found a T3/T4 combo seemed to turbo charge me - and I couldn't find a balance :
I find NDT much softer on my body and the fixed ratio suits me.
I simply dose to the relief of symptoms as originally used and not to a blood test, or a range or a guideline.
NDT was used successfully for over 100 years long before the advent of Big Pharma's T3 and T4 tablets launched on the back of NDT and the introduction of the blood tests, ranges and guidelines that we are all meant to fit into.
NDT contains all the same known hormones as that of the human gland so I'm replacing as best as I can, like with like.
It's ironic really as in Toft's 2017 article he actually questions RAI thyroid ablation for Graves Disease - which is what I was treated with - and which was the worst decision of my life, though hardly a decision as I wasn't even given any choice and didn't know enough back in 2005 and simply trusted that the medical profession knew best and " first did no harm " :
The TSH doesn't cause symptoms - it's simply a signal from the pituitary to stimulate the thyroid and if you've a problem with your pituitary you'll have trouble being dosed to wellness in primary care as the knowledge and skill set isn't there.That’s interesting so you’re saying I could have a problem with my pituitary gland? As far as I’m aware, it doesn’t take too much T4 to suppress my TSH.
Yes, fighting the NHS on this doesn’t seem a good idea because I don’t think the doctors really know what they are doing. After Dr Toft retired from the NHS, I saw his replacement. It didn’t go well. I came away after the second appointment in tears and decided to look for an alternative. It was then I discovered Dr Toft worked privately.
Definitely there is a problem, but I’m not sure what it is. Dr Toft likes TSH to be in range when on T3 and T4. I have no idea how to get mine there!
With NDT, how do you know you are taking the same dose every day? Is it not hard because you don’t know what’s in it? As in the levels of each hormone.
I need to do lots of research so I can help myself. It’s great you are so confident self medicating. One day I hope I am too.
No, it's very simple - each tablet, referred to as grains, contains trace elements of T1. T2 and calcitonin plus a measured dose of T3 and T4 :
Each grain of my NDT contains 9mcg T3 + 38 mcg T4 : and you need a pill cutter.
I stopped 125 mcg T4 one day and started on a quarter of a grain of NDT the next day.
It takes around 6-8 weeks for the T4 to totally leave the body and in that time you slowly build up your NDT level in weekly 1/4 grain increments and monitor blood pressure, pulse and temperature twice daily.
There will come a week when you don't feel as good as the previous, maybe a little edgey and uncomfortable in yourself so you drop back down to the previous weeks dose, stay on that 6-8 weeks letting it settle and bed in and then you take a blood test to track where you are and compare to your bench mark readings and if well, this is your best dose on NDT at this point in time. and your T3 has likely moved higher than when on T4 monotherapy.
If you get to 2 grains it's suggested you give this dose 6-8 weeks to bed in and then get a blood test just to compare with your bench readings before switching to NDT :
If you feel ok, but still have some symptoms, and your T3 has moved and going in the right direction but not high enough for you, as you still have symptoms, you start off again, building up in 1/4 increments from 2 grains until you go a little too far, and then you drop back down that last 1/4 you increased.
NDT is subtle, and it can take time, though I found immediate benefits of my brain waking up and cognitive functions improving, and other symptoms that I just " lived with " started o disappear long after I started NDT and I realised around 18 months in, the other bonus was loosing around two dress sizes,
When optimally medicated you will likely have a low suppressed TSH : you may well have a lower T4 than from when on T4 monotherapy BUT your T3 should be proportionately much higher to when on T4 monotherapy.
On T4 monotherapy my T3 was around 25% with a T4 at around 100 / 110% :
On NDT my T3 is now at around 90/110% through with a T4 at around 25% :
My temperature rose from 35.4 to 36,6 which is ok for me my pulse and blood pressure remained constant and I am much better than how the NHS left me.
Trust that all makes some sense - I'm way past my best before time of day !!!
That does make sense and thank you so much for explaining how you did it. It’s extremely helpful if I go down the NDT route.
At the moment, I’m not sure what to do but know I need to do something. My voice, after being not too bad, had become worse again. The more tired I am, the worse it is. I really hate it!
Are the grains like a pill? And you have a pill cutter?
Thank you very much again for explaining it all so clearly and well.
First step is to get FULL thyroid and vitamin testing
Were latest thyroid tests done as early as possible in morning before eating or drinking anything other than water and last dose levothyroxine 24 hours before test
Do you always get same brand levothyroxine at each prescription
Many people find different brands are not interchangeable
Do you know if your hypothyroidism is autoimmune thyroid disease also called Hashimoto’s diagnosed by high thyroid antibodies?
ESSENTIAL to regularly retest vitamin D, folate, ferritin and B12
For good conversion of Ft4 to Ft3 we need OPTIMAL vitamin levels
What vitamin supplements are you currently taking
With low Ft3 low vitamins are almost inevitable…..low Ft3 results in low stomach acid, this leads to poor nutrient absorption and low vitamin levels as direct result
The test was sprung on me as I had made an appointment to see the doctor about something else. He decided to do some blood tests himself. It was done at around 11.45 am and I had eaten breakfast. I take my thyroid medication (always Eltroxin) at night and I didn’t take it the night before. So it would have been more than 24 hours since the last dose because I take it at night.
I don’t have high levels of antibodies as far as I’m aware. Dr Toft tested them and said I had some, but that most have some, but they weren’t high.
At the moment I am not taking any supplements. I didn’t think they were a good thing. But they are, obviously, otherwise you wouldn’t ask which ones I was taking.
It’s interesting what you wrote about T3 and stomach acid. I had no idea. I’m going to do some research.
Once I have my results, I’ll post and see how I can best optimise them.
Thank you very much for taking the time to help me.
Important to test BOTH TPO and TG thyroid antibodies
NHS only tests TG antibodies if TPO antibodies are high.
Most people with autoimmune thyroid disease have high TPO or high TPO and high TG antibodies…..but a significant minority only have high TG antibodies and won’t get diagnosed by NHS testing
Are you on strictly gluten free or dairy free diet
Both these tend to lower TPO antibodies
Have you ever had ultrasound scan of thyroid
20% of Hashimoto's patients never have raised antibodies
I will look back and see if I have the test results although I am not sure I ever got them. It was Dr Toft who did the tests. It was years ago now. I cannot understand why the NHS is quite so awful when it comes to thyroid. It seems as though they don’t do the very tests than need to be done.
I am not gluten or dairy free. I would find it terribly hard to be so. I’m vegetarian but would rather not be vegan.
The present review of the literature regarding B12 status among vegetarians shows that the rates of B12 depletion and deficiency are high. It is, therefore, recommended that health professionals alert vegetarians about the risk of developing subnormal B12 status. Vegetarians should also take preventive measures to ensure adequate intake of this vitamin, including the regular intake of B12 supplements to prevent deficiency. Considering the low absorption rate of B12 from supplements, a dose of at least 250 μg should be ingested for the best results.3
Low iron and/or ferritin
Extremely important to do full iron panel test for anaemia including ferritin
Likely low in ferritin, possibly low in iron on vegetarian diet and Hashimoto’s
It’s extremely difficult/impossible to maintain GOOD iron/ferritin on plant based diet without supplementing
Strongly recommend getting full thyroid and vitamins tested via Medichecks or Blue horizon
I have the results now so I will post separately so that I can see how they are. I don’t know how to interpret them but hopefully after some help, I will!
I eat cheese and drink milk and I try to have a lot of pulses and beans etc.
I was stable on 200mcg for 6yrs, but since May 2018 I have gradually reduced to 112.5mcg. Last reduction of 12.5mcg was Aug '21. My weight has been stable at 60kg for the past 7 yrs. My conversion is a bit better than yours. I am 62 & Hashi's for 14 yrs.
The only anomaly for me was a coeliac dx in Nov 20. It makes no sense 'cos you'd think (and anything you read will tell you) with malabsorption issues Levo requirement would increase. Of course, the 200mcg at 60kg was a fairly whopping dose, which on reflection, maybe should have raised questions, but during that period my TSH averaged 2 & FT4 17.5..........
If you find the answer to why your Levo requirement has so substantially reduced I would love to know.
nb I was tested for coeliac at Hashi's dx in 2007 which came back negative
SlowDragon, my Levo reductions from 200mcg to 112.5 were all in the 3 yrs leading up to the coeliac diagnosis (apart from the last 12.5 mcg) so I wasn't gluten free, and in this context improved absorption due to gf diet is not applicable.
Consistently low since 2007..........I was really quite angry when I got on-line access and realised. Much better since Apr 21, although they won't be good at the moment. I'm having a bit of a hic-cup with my gut, and haven't taken any supplements since Dec 21.
I expect vits/mins can make a huge difference, or a minor difference. I agree its worth bearing in mind.
12nmol. Oooh, I hate to imagine how bad you felt. I'm curious, did it have a range on those old results? Mine hadn't been tested at all before last year.
Oh, I assumed it must have been prior to the introduction of these measurements, but I don't know how long they have been in place, and of course the range is only visible when you drill into 'comments'.....under the space for range it says N/A.
The 'comments' also over-write after each new test, unlike 'Range' where you can clearly see historic changes.
I'd assumed that not so long ago the range would have been <25, and that change was forced. Either way, not doing something about your 12 is unforgivable.
It’s trial and error what dose we need, with hashimoto’s we frequently need higher dose than average
I found by regular testing over last 8 years…I need 4000iu daily as maintenance dose in summer….5000iu in winter. Took 3-4 months at 6000iu to increase dose up to decent level.
But we are all different….Many people wouldn’t need anywhere near that high a dose
I have Hashimoto’s and gluten intolerant (tested negative for coeliac….more on my profile)
I now have all my blood test results. I’ll post them separately to see how they are. I’m not really sure because I am not sure what to look for.
The doctor didn’t do my Vit D so I will start supplementing and then have it done as you suggest - late winter and late summer.
With my thyroid results it looks as though the T4 has gradually got higher and the T3 has gradually got lower. My dose has gradually got lower as my T4 got higher. I am now on 125mcg.
The best way to get access to current and historic blood test results is to register for online access to your medical record and blood test results
UK GP practices are supposed to offer everyone online access for blood test results. Ring and ask if this is available and apply to do so if possible, if it is you may need "enhanced access" to see blood results.
I rang the surgery and they have done it for me. I have everything from July 2016 when we moved back to the UK from France. Thank you for your suggestion.
Too many reasons to accurately pin it down probably, and likely attributed to whatever was the most 'fashionable' thinking at the time. From what I've read, Dr Toft was the advocate for not being concerned with over range T4, as long as T3 is in range, and this seems to be very effective for many people, but maybe the improvements he saw in his patients using this protocol blinded him from seeking other reasons.
Who knows? Maybe, in 5-10yrs we'll be back on 200mcg, without ever knowing why we took a long dip. I am now keeping an eye on trends in all my blood tests.
I would recommend that you investigate your gut though. I had classic symptoms, but many more people are being diagnosed coeliac without gut issues, but have either low iron, or neurological symptoms leading to further investigation.
It's easy to switch to gluten free when you've had the classic symptoms, and then discovered what the problem was. I would have found it incredibly difficult if I hadn't felt so unwell, or had a positive coeliac dx.
I used to go to my local bakery just about every morning for a fresh coffee and warm almond croissant. It has taken me about a year to look longingly at them again. 🤣 It's fresh bakers bread I miss the most though. I dream about the perfect sandwich.
In your shoes, I'd start with testing Iron. Folate, B12 & vit D, and if these are OK look at T3. If they're not OK look for any gut problems.
I used to make fresh bread every day. It was divine! I guess if you feel unwell with it, it’s not going to be too hard to give it up. There don’t seem to be many good alternatives.
I hope one day you find the perfect GF almond croissant. And bread!
Edit ...This is a bit of a ramble , forgive me, i stayed up too late watching the northern lights and seem to have lost track of any point i was making ... but you never know ..it might still be interesting
I've ended up on less Levo as the years have gone by too. (I became hypo during my 2nd pregnancy, aged 32 with autoimmune hypo)
I was on 150mcg for 13 yrs. (dose by weight would have indicated only 100mcg ish , but i felt naff on 100mcg )
Then ? around the time of beginning of menopause aged 49/50 ish , i developed all sorts of random problems, eg . horrible pain like kidney stones , calcium oxalate crystals in urine but no kidney stones found , and i'd developed symptoms of overmedication. eg slight tremor in fingers , jumpy, worsening of sudden onset fatigue/ crashes , weight loss , over frequent bowel movements etc. ( first GP didn't check thyroid bloods or consider thyroid at all... doh ! )
So, had colonoscopy /endoscopy .. no sign of coeliac/cancer etc .
Dose was reduced to 125mcg (by 2nd GP, who used her brain) which slowly improved things. (dose reduced due to symptoms and because my fT4 was a little bit 'over' @ 110% through range . It had sometimes been higher than that before , without it causing me any issues., but my 'usual' TSH of 0.05 had fallen to 0.01)
I was then ok on 125mcg for 3 yrs ,
Then different GP asked me to reduce to 112.5mcg , even though i felt pretty good at the time (because fT4 had gone up to 200% through range, TSH was still my 'usual' 0.05 ish) ..... this reduction caused problems ..... i became too knackered to do much work.
3 months later , GP asked me to reduce further to 100mcg (because fT4 had unexpectedly gone UP again , to 240%, but TSH had risen slightly to 0.09 as expected)... GP confused .... he asked if i'd increased my dose by mistake , but i hadn't .
Eventually , due to concern about the silly fT4 levels, i did agree to reduce to 100mcg over 3 months , but in the end i spat my dummy , cos my digestion ground to a halt, chronic constipation, and my brain was struggling to even cross the road safely , so even though my fT4 was still 180%, (TSH up to 0.5) he put my dose back up to 112.5mcg. .. and my digestion worked properly again, constipation resolved , and i slowly felt better.
I'm still on 112.5mcg now (2 yrs later ) and my fT4 did come down a bit more , even though the dose was put back up , (last test it was 140%, and TSH was higher than my usual at 1.9)
I don't have any solid explanation for why my fT4 did this, or why my dose is less ..... it's hard to say which came first ...chicken /egg :
eg. I 'use' less Levo now , but i also do a LOT less physical work now ...and i don't really know which came first.
But 'less activity' can't explain all of it ....was still doing loads of work when i became overmedicated on 150mcg , and i was still doing just as much work on 125mcg when i felt OK but fT4 had gone through the roof.
Menopause might have been a factor (estrogen has a relationship to thyroid hormone transport /binding ) ..... and there was a bit of nervous breakdown somewhere it the middle of this lot too....
I've stayed on 112.5mcg mainly cos i realised i was sleeping better, and curiously my recurring lifelong backache had totally gone away ... but i'm also much less physically active now than i was when on 125mcg..... so maybe i just don't push my back so much anymore cos i don't do so much work ?
So I've pretty much 'retired' myself , and now i can do silly things like sit up till 5am watching pretty lights ... and waffle aimlessly on here.
So anyway .... it's not just you that doesn't know why your fT4 is higher than it was .
But be open minded .... sometimes a reduction in dose can be an improvement , and sometimes it isn't.
You have certainly been very up and down. Even more so than me.
It’s interesting that you have never taken NDT or T3. It’s all been T4. That’s the same as me.
I reduced to 125mcg when my voice became too much of an effort and that has helped slightly - unless I’m very tired.
I have not been feeling great for quite some time and I’m sure it’s thyroid related. But I’m not sure in what way. Perhaps T3 would make a difference. But in the Toft Talks video he said that in order to take T3, your TSH needs to be within the normal range. I’d have no idea how to get mine there! I guess I’d have to reduce the Levo by quite a lot, and I’d end up feeling even more dreadful.
my gut feeling is that Toft, and many others public statements on ' get TSH in range before adding T3' , is probably more to do with covering their back (in light of all the controversy, and the GMC hounding those prescribing it) not because it's necessarily a better idea for everyone . I think they feel on safer ground agreeing to T3 use in clear cut cases where very low T3 is evident , and where 'in range' TSH means no one can argue overmedication with Levo or T3 is the real cause of the presenting symptoms or any later problems .
Not because it's true , or even what they really think, but because the 'TSH is Infallible' theory, has become so dominant that "in-range TSH" is now a professional 'safety net'.
But that limits T3 treatment to a very few cases who happen to have that nice 'safe' level of TSH response to their hormone levels.
It all seems a bit 'catch 22' to me .... "You can't have T3 if your TSH is below range on Levo , because that means you're overmedicated on Levo , so lets fix that first".
" You can't have T3 if your TSH / fT4 / fT3 are in range on Levo , because that means thyroid isn't causing your problems anyway , so go away."
"You can only have T3 if your TSH and fT4 are in range but your fT3 is below range."
......... which is fine for the 1% of patients who happen to have those results , but no help for anyone else.
And insisting TSH is in range first , seems a bit pointless anyway .... because even those people who did have in-range TSH when T3 was prescribed will often end up with TSH well below range as soon as you add T3 ... so then they take it off them because their TSH is supressed .
I bet there aren't very many people feeling well on Levo + T3 who's TSH is still in range ... not if the results we usually see on here are anything to go by.
A few will be lucky and TSH will stay more or less in range, but that doesn't mean its possible for everyone else to get their TSH to co-operate so nicely .
I'd definitely consider lowering a high ft4 a bit before adding T3 , i'd try a lower dose Levo for a few months just to say i'd tried it properly , and use that time to improve anything else that wasn't optimal ..... but other than that, i wouldn't let a low TSH stop me from adding T3 if i wanted to try it .
Having said that , if you're interested in getting your TSH to come up a bit without altering your dose .... An interesting experiment might be to try splitting your Levo dose into 2 doses (morning and night) the idea being that lessening that big daily spike of T4 from one dose, might just allow TSH to rise a bit ..... there's no proof for this theory , but perhaps worth the experiment .... i do it now , and coincidentally (or not) ... 6 months later, my TSH was 1.9 for the first time after 20 yrs of 0.05 ish .
I now do 50mcg before breakfast /62.5mcg before bed .
( this also has the useful side effect of stopping you eating Maltesers all evening after your dinner, since you need a few hours after food before the bedtime Levo dose )
Thank you very much for the long and detailed reply. There’s a lot to digest.
My TSH has been suppressed since the beginning, 18 years ago this summer. I have never heard of the splitting the dose. What an interesting experiment that would be! Do you know why it would raise your TSH? Did it do anything to your T4 or T3?
I think I could try that. I take 125mcg. So I could do it 50/75. I could take 50 in the morning and 75 at night. At the moment, I take it all at night. The only difficulty I might have is remembering!! I have the worst memory ever. But I could set a reminder on my phone.
When Dr Todt suggested T3, I don’t recall him suggesting I lower my TSH. He did say the Eltroxin would be lowered.
If I were to add in T3 at some point soon …. I will finish later. My dog needs to go to the vet.
Start with looking at vits .. and use the time to read more on here , so you understand how everything 'thyroid' works . (makes it easier to spot 'Bullshit ' if you do later choose to see an Endo)
Different Endos' have different ideas on when they will /won't prescribe T3.
~ Some will prescribe when TSH is below range .
~ Some won't .
( i'm sure some people on here have been prescribed T3 even by NHS endo's ,when TSH was a little below rage.)
~ Some indicate they might .... once you've done this that or the other with your Levo dose (re-arranged the deckchairs on the titanic lol).... but never actually do, no matter what your result are once they've finished fiddling about with your Levo dose for 6 months .
I'm very jealous of the Northern Lights watching. I'm down S'arf.
There are definite similarities to our histories. I couldn't maintain your high FT4 though, but then I was older at 48 when diagnosed, my periods had stopped about 6 months prior, and although I worked long hours I sat at a desk all day.
I had an endoscope in 2010 which was clear. I'd bet £1 to a penny that I was coeliac then. Most of the time they've got to be specifically looking for it to find it. Never had a colonoscopy, but I have a feeling it might be on the horizon. 🥴
i am "up norf ", so i might well have been able to see them... 'cept a) it was cloudy.. and b) some inconsiderate sod keeps building towns and leaving the streetlights on . .......however , thanks to a camera run by some polar bear scientists, i was watching them over Hudson Bay .
i'll give you the link if you want , but don't blame me if you end up staying awake till 5am too. Its very dangerous .... once you see them you can't go to bed till they stop .
Ah, I saw a news report a couple of days ago ( I think it was a couple of days ago....although, you never know, could have been much longer) about 'lights' being visible up north..........so, just assumed.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")