I have been getting results where my T4 and T3 are hardly through mid range but my TSH has been suppressed. As a result my endo.reduced my dose to 50mcg of levo and 15 mcg of T3.
While this slightly improved my TSH (just close to the lower end of the range) my T4 and T3 were close to the lower end of the range.
I started loosing a lot of hair, felt extremly weak and fatigued and started getting the feeling that I'd faint anytime.
I increased my levo to 75mcg and stopped my T3. This didn’t help either.
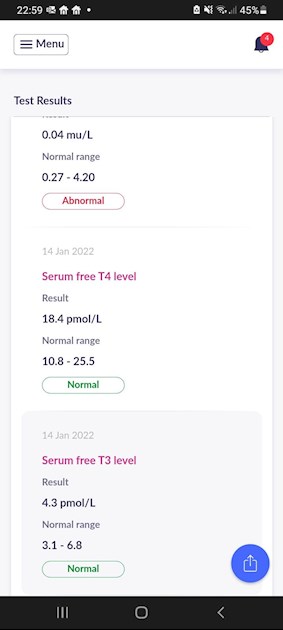
So over time I increased my levo to 100mcg with no T3. This made me feel much better. The feeling of weakness and feeling faint went away. I feel much more energetic and my hairloss has improved. However, it comes with a suppressed TSH - results per attached.
As you can see;
1- My TSH is suppressed
2- My T4 is 52% within reference range
3- My T3 is 31% within reference range.
I fear my endo will advise me to reduce my levo given the suppressed TSH.
Are there any people on this platform who have the same issue and if so, how have you dealt with this please?
What's the downside of suppressed TSH? I have heard from my endo that it leads to osteoporosis and heart issues. Is there any reliable evidence of this?
Also, would you advise me taking T3 seeing my T3 values?
Many thanks for your help?
Written by
New2thyroid
To view profiles and participate in discussions please or .
There you will find a very large, long term study of patients on Levothyroxine, showing the risk associated with TSH 0.04 to 0.4 were no greater than the risks associated with TSH 0.4 to 4 (ie. 'in range ' )
There are also links to several other good posts discussing the subject of low TSH /risk.
Great info from tattybogle, and in rely to your question yes, this issue is one of the big topics on the forum.
When we are hypothyroid there are many reasons why our TSH fails to correlate with expected levels of thyroid hormones and until doctors stop dosing solely by TSH values, many risk remaining under-medicated.
Thyroid hormones need certain cofactors to be adequately met in order to work effectively. The most common deficiencies negatively effecting our meds are low levels of VitB12, folate, Vit D and iron, and therefore it is difficult to suggest meds doses or combos until you are certain these have been met.
Thanks so much Tattybogle! Very grateful for your help. I wonder if I should reintroduce T3 along with 100mcg levo (as didn't feel great with 75mcg levo +.15mcg T3).
personally i'd suggest that if you feel improved on 100mcg Levo , you stick with it for a bit longer to see if you continue to gradually improve over the next few months, before considering re introducing T3 to the mix. You might not need to , and if we can do without it it makes life with the GP much simpler.
I think, where thyroid hormones are concerned, there is a lot to be said for stability.
And also the old addage " if it ain't broke .... "
I know from my own experience when staying on a dose of Levo that initially only gave slight improvements in some areas ... that i actually felt increasingly better in several other areas over the next 6 months on the same dose. I had been tempted to change something , but in hindsight i'm glad i gave it longer.
Your immediate challenge is to persuade your prescriber to ignore the low TSH and keep levo at 100mcg ..... Adding T3 at this stage will only make that challenge harder .. because TSH will almost certainly fall a lot lower once T3 is added.
Are your tests done with leaving a 24hr gap before the T4 test and 8hr gap before T3 test. If so, when you do your tests it’ll be much lower than if you took a test just after taking either Levothyroxine and/or Liothyronine. Your TSH could be suppressed if you spike over range for T4 and T3. Which indicates you’re on slightly too much medication. Have you considered using liquid Levothyroxine? You can alter your dose ever so slightly rather than in 25mcg reductions. Although there is one brand that does 12.5mcg size tablets. I’m using liquid Levothyroxine and needed to reduce my Levothyroxine by just 10mcg a day. It’s so easy to do so with the liquid. You can even drop it by 5mcg if you want. Or increase. My NHS Endo said he’d stop prescribing T3 if my TSH went suppressed!! Idiot I thought. He’s needs to help me manage it, not withdraw it. Anyway I helped myself by trial and error. I found best way for myself was to reduce Levothyroxine ever so slightly and not change my T3 dose of 5mcg twice a day. T3 is your main requirement.
I know this doesn’t answer your question about suppressed TSH and what that would do to you long term. I now can keep my TSH at a good place just within range. Last test it was 0.64(0.35-5.50). And to be honest I feel much better when I’m lower part of normal.
My sister, who had thyroid cancer, always has to keep her TSH suppressed. She has never been warned about any ongoing issues from her Endocrinologist about heart or bone issues or anything. So, I’d also ask your Dr why are cancer thyroid patients not warned about these issues and others told not to suppress. I know they choose to suppress thyroid cancer patients to stop any cancer returning but why don’t they warn them too. It is an argument that you could mention to your Dr next time.
From your results I’d say take T3 but only small dose and also take twice a day leaving 8hrs apart. You could compensate with a reduction of 10mcg Levothyroxine to start with. It’s T3 that your main requirement. Request liquid Levothyroxine to help you manage your intake. Unfortunately it’s all trail and error as we are all so different. During a trial you need to keep each trail steady for at least one week for your body to adjust. Then continue for another week unless you feel awful of course. Always get blood test done as often as you can. My GP always have me a spare blood form so I could get my bloods done if I had negative signs so I knew what was going on. Sometimes I’d be over medicated. Sometimes I’d be under. It was striking the right balance then sticking with it methodically. Routine is key.
Thanks so much McPammy. It was a 24 hour gap for my T4 and T3. Would you know if the liquid Levo is available on NHS Please? Do endos prescribe it freely? I think I would like to try your approach of reducing my levo to probably 90mcg and reintroduce my T3 to perhaps 10 mcg (split in two).
Yes, I get my liquid Levothyroxine from my NHS GP. It is more expensive than tablet form and may have to be authorised by the medication manager at your surgery. It’s good for some, not all, to split your T3 dose 8hrs apart. Some take it 3 times a day. My private only Endocrinologist prescribed liquid Levothyroxine also for myself and asked my GP to prescribe it through the NHS. My GP agreed along with the medication manager.
I’m a poor converter of T4 to active T3 that’s why I need my T3 every 8hrs otherwise my conversion from Levothyroxine is too low. I now feel bloody marvellous to be honest.
I hope you get the liquid Levothyroxine, even for a trial request initially would be good so you can check.
Any questions I’m always pleased to help if I can.
Sorry I misunderstood. Previously when I have been on T3 I gave a 24 hour gap but I am not on T3 anymore just on 100mcg levo.for which I left a 24 hr gap. The blood results are only with 100mcg levo. I stopped taking T3 as I upped my levo from 75mcg to.100mcg and didn't want to overexcited myself by keeping the 15 mcg of T3 (which I was taking along the 75mcg levo). Surprisingly, I felt much better on 100mcg levo vs 75mcg levo + 15mcg T3.
Hi greygoose hope you don't mind me replying to your comment after span of ten months. I so appreciate your wealth of knowledge and hope you have the time to answer my query. Recently, I had thyroid test and considering your comment above, regarding FT3 my test result is false based on time of last dose of T3. Day before test I took levo 6am NDT at 5pm. No levo on day of blood draw which was taken at 10am, 17 hours after my last dose of NDT!!!!! My FT3 result was 5.4 3.1-6.8. Taking time factor of last dose of T3 into account would this indicate that FT3 of 5.4 would/could have been higher, or even lower if I had done blood draw within 8 to 12 hour time line?
If you'd left the recommended gap of 8 to 12 hours between the last dose of NDT, and the blood draw, your FT3 would most certainly have been higher. Although impossible to say by how much.
Yes, you have confirmed what I suspected after reading this post and comments, specifically your one. Sincere thank you for clarifying this query for me.
I completely agree about very finely adjusting doses of Levo to try and keep TSH from being totally supressed, if possible, (for some, who's TSH sits lower than yours, it isn't possible without feeling undermedicated) . But prescribing liquid Levo is very expensive and simply won't be allowed for most of us unless we are having an issue with all brands of Levo tablets.
12.5mcg tablets are also very expensive, (and only Teva make them) , but due to the long half life of Levo , very fine adjustments can be made very easily using standard 25mcg tablets, simply by having slightly different doses for a few days a week, or halving them to get 12.5mcg etc .
eg .
7 days x 100mcg =100mcg /day
(5 days x 100mcg) + (2 days x 75mcg) =92.8mcg /day
They invent this stuff about hearts and bones to scare us off. There is no evidence that TSH leads to problems. It's a pituitary hormone not a thyroid hormone. You can have issues with over range FT3, but it needs to be considerably over range for a prolonged period.
When we take T3 meds, our TSH drops. That's just what happens, and if your endo doesn't understand this (a) s/he prob should find a different job and (b) s/he will keep you ill ....
You are ONLY over-medicate when free T3 is over-range, not when TSH is low; and it is ONLY dangerous to have suppressed TSH when (a) you are not on thyroid meds AND (b) this is accompanied by free T3 that is waaaay over-range x
This makes sense in terms of my medical history so far and would explain my TSH levels. Wonder why endos are so obsessed with the TSH numbers. Thabks so much fuchsia-pink!
" it is ONLY dangerous to have suppressed TSH when (a) you are not on thyroid meds AND (b) this is accompanied by free T3 that is waaaay over-range x "
I accept that it is too long a reply to give in most cases when this question is asked , but i think the truth re. supressed TSH /risk on Levo only is more nuanced than your statement implies.
The study i use obviously can't be applied to those taking T3 ,as that would affect TSH in a different way to Levo only..... but personally I found it more helpful when discussing Levo only dose with GP's , to accept that there is evidence for some risks, but to make sure they are put in their proper perspective .
Denying that there is any evidence for any risk at all , at any level of TSH suppression, is perhaps counterproductive , i suspect it just makes GP's think we don't know what we're talking about.
I think , at least when talking to patients on Levo only, that we should be clear that there is some real life evidence that there may be some increased risks in patients on Levo who's TSH is actually supressed below 0.04 but that it needs to be looked at in context by pointing out that the increased risks associated with heart an bone for supressed TSH were mostly less than the increased risks associated with TSH over 4 ...( which the NHS is not remotely concerned about since they happily accept the risks of leaving people until TSH is over 10 before treating them.)
There are acknowledged limitations with this study , "It is unfortunate that we did not have access to serum free T4 (or T3) concentrations in these patients to ascertain whether they were above or within the laboratory reference range." , but it's methods and objectives seem fundamentally sound to me, and it is looking at real patient outcomes over many years. I think judging by the many full blood tests we see here on the forum that it is reasonably safe to assume that not many, if any, of these patients on Levo only will have had T3 that is 'way over range'..as this is usually very hard to achieve using levo only.
"Design: We conducted an observational cohort study, using data linkage from regional datasets between 1993 and 2001.
Setting: A population-based study of all patients in Tayside, Scotland, was performed.
Patients: All patients taking T4 replacement therapy (n = 17,684) were included.
Main Outcome Measures: Fatal and nonfatal endpoints were considered for cardiovascular disease, dysrhythmias, and fractures. Patients were categorized as having a suppressed TSH (≤0.03 mU/liter), low TSH (0.04–0.4 mU/liter), normal TSH (0.4–4.0 mU/liter), or raised TSH (>4.0 mU/liter).
Results: Cardiovascular disease, dysrhythmias, and fractures were increased in patients with a high TSH: adjusted hazards ratio, 1.95 (1.73–2.21), 1.80 (1.33–2.44), and 1.83 (1.41–2.37), respectively; and patients with a suppressed TSH: 1.37 (1.17–1.60), 1.6 (1.10–2.33), and 2.02 (1.55–2.62), respectively, when compared to patients with a TSH in the laboratory reference range. Patients with a low TSH did not have an increased risk of any of these outcomes [hazards ratio: 1.1 (0.99–1.123), 1.13 (0.88–1.47), and 1.13 (0.92–1.39), respectively].
Conclusions: Patients with a high or suppressed TSH had an increased risk of cardiovascular disease, dysrhythmias, and fractures, but patients with a low but unsuppressed TSH did not. It may be safe for patients treated with T4 to have a low but not suppressed serum TSH concentration."
" Compared with a normal TSH, suppressed serum TSH was associated with a modest increase in cardiovascular morbidity and mortality, whereas high TSH was associated with a near doubling in risk. There was no significant difference between low and normal TSH levels..... A similar situation existed for dysrhythmia admissions, although the risk associated with a suppressed TSH was nearly as large as with a high TSH concentration. Again, there was no significant difference in outcomes between patients with a low TSH and a TSH in the reference range. Suppressed TSH was associated with a doubling of the risk of osteoporotic fracture, whereas the risk of a high TSH was only marginally less. There was no significant increased risk associated with a low TSH."
It's a puzzle isn't it, I did a private test in December and had a TSH of 0.03 but thyroid hormones of only 50% through range. I use supplements for Vitamin D, folate, B complex and a separate B12 spray. I'm worried when it comes to getting an NHS test my GP will reduce my dose of Levo. I've nothing useful to add except you have my sympathies.
HiI don't see an Endo, but hearing about the stories on the forum about stupid so called specialists maybe that's no bad thing. Dealing with one less optimally informed medical expert (GP) is one thing but two?
In one sense it's like asking "how long is a piece of string?" That is it depends on the circumstances - suppressed TSH dangerous in hyperthyroidism, but not necessarily in treatment, to which the body reacts totally differently. Without a working thyroid, and taking T3/T4 combination, the gland (hypothalamus) that stimulates production of the pituitary (TSH) the T3 has a disproportionate influence. It inhibits the hypothalamus so that the signal to make more TSH doesn't occur and it therefore is suppressed. But this is nothing to do with the FT4/FT3 levels needed for bodily health, which are controlled by what you take in. To a large extent TSH is "offline" in the cascade of reactions - that is, it no longer has safe signalling properties, and so should not be the arbiter of the optimum dose.
Suppressed TSH can be dangerous but this doesn't appear to relate in any way to your circumstances.
TSH is a pituitary hormone, not a thyroid hormone, it reflects the level of hormone in the blood which is why it is currently considered to be the " gold standard" test.....however it does not tell the whole story and therein lies the problem.
The most important lab is FT3....that is the free or unbound T3 in the blood which providing that the patient has no form of Thyroid Hormone Resistance - RTH ( fairly rare and the problem I have) will then be transported the nuclei of the cells where it becomes active.....and if the supply is adequate and constant will keep you well.
So long as FT3 is in range you are not overmedicated. Those of us with RTH need higher doses of T3 so FT3 rises above range and FT4 and TSH becomes suppressed - both my TSH and FT4 have dropped off the lab scale but I'm fine.
Unfortunately we hear scaremongering tales of osteoperosis and heart problems being caused by low TSH
Research proves otherwise - remembering T3 can lower TSH, depending on size of dose
The use of the words "Normal" and " Abnormal" is also open to misinterpretation because they refer to results being in or out of the range which is only part of the story. What we need to find instead is the result that is optimal for each individual and that is the point/ number on the scale where one feels well....a result somewhere in the ref range is not good enough... we aim for a specific point!!
Why were you prescribed T3?
Poor conversion? High FT4 with low FT3 is the normal sign but that's not entirely obvious with your current labs because we don't know the values of the following co-factors
Did your endo point out that vit D, vit B12, folate and ferritin need to be optimal in order to support thyroid function / conversion of T4 to T3. I doubt it!
I would suggest that is the first thing to do is test the above nutrients then supplement if levels are low
I'm assuming the above results were with 100mcg levo only - see quote below
With T4 only 52% through range you first need more levo
FT4 and FT3 should be approaching 75% through the ref range!
That increased levo should convert to T3 and raise your FT3
So over time I increased my levo to 100mcg with no T3. This made me feel much better
Until both of those things ( nutrients and more Levo) have been done I would not add more T3.....if indeed you need T3. But meantime hold tight to your T3 and to your T3 prescription, it will not be offered again! I have to buy mine myself.
Your endo has poor thyroid knowledge....most likely a diabetes specialist.
So don't worry about the TSH, instead, I'd suggest ensure your levo is increased by 50mcg, retest in 6/8 weeks then, depending on labs , repeat this until you feel well.
Your T3 dose may also need to be reviewed ...but one thing at a time
Bottom line, TSH is not the gold standard route to find one's therapeutic dose.
Post your new lab results and members will help
I'm not a medic, so not qualified to advise, and know only what my own reading and research has uncovered via a long and bumpy thyroid journey that eventually revealed that I have a form of RTH and need high dose T3 to function....medics couldn't help me!
Hi Dippy, perhaps i'm being overly cautious this morning , but I do wonder if increasing Levo is really needed at this point, based on this comment :
" ........ 100mcg with no T3. This made me feel much better. The feeling of weakness and feeling faint went away. I feel much more energetic and my hairloss has improved. However, it comes with a suppressed TSH -"
I don't think it's a given that 'fT4 and fT3 should be approaching 75% through the range '.. anymore than anything else about thyroid hormone replacement is a given.
Might it not also be the case that if improvements are already felt on 100mcg , they might well continue if the dose is left alone to allow stability? .
Whereas pushing to increase dose to 150mcg might well destabilise any improvements that are going on currently .. and will certainly be a difficult ask to get the GP to agree to.
Not that we should be making life easy for GP's of course ,, but also we surely shouldn't assume everyone will improve further with T4/3 @ 75% if they say they currently feel improved at 52% ?
It was being cautious that resulted in it taking a veeeery long time to find my therapeutic high dose of T3-only.
I absolutely wasn't suggesting "pushing the dose to 150 mcg" as you suggest...I mentioned a 25mcg increase and suggested in time a further increase may be an option.
Edit Argh! That was meant to read increase by 25mcg, not 50mcg......you' re correct about that! Blunder!
I realise 75% through ref range is not for everyone and certainly not "a given"....I said approaching 75%
Approaching 75% is just that...."approaching"!
I wasn't assuming anything, just pointing out that 52% may not be adequate in this case and a number approaching 75% may be better. 60% for example...
So over time I increased my levo to 100mcg with no T3. This made me feel much better
Much better - That is improvement, but she still doesn't say she feels well
Improvement is not cure.
Do we actually know how long she has been on this dose....perhaps that's a question that needs to be asked
I'm not convinced she needs T3 at all and it looks as if the T3 has been "helping" to suppress the TSH which has been giving (unnecessary) concern.
With the T3 removed ( as has happened) it's likely that in time levo will need to be increased.
We need timescales.
I am absolutely no expert tatty, and would never claim to be, I'm just like everyone else here, doing the best they can to improve their lot.
When I arrived here in 2017 I could barely function, medics had no idea what was wrong with me, the one endo I saw said I needed to keep taking levo...which after 20+ years had left me in that state.
I was convinced this was a thyroid problem - I told one patronising GP that I intended to find the answer - because numerous scopes, scans treatments and medications both NHS and private showed no other problems... but improved nothing.
It's been a challenging journey and at 76 I am now much improved though some of the damage done, over possibly a lifetime, leaves traces of some of my former and many symptoms.
I did find the answer. I have a form of Thyroid Hormone Resistance that causes low cellular T3 - that is cellular rather than glandular hypothyroidism and to function I need high dose T3-only ( currently 87.5mcg it has been 212mcg ) This is thanks to the help of amazing people here and by reading books and searching on the internet....had I not, I may now be dead instead of getting on with life.
Thank you TUK!
I'm sorry if you feel my ideas were misleading....I'm always very happy to be set straight if I make a blunder. Something we all do occasionally.
However, if you are suggesting that , I ,or in your words, we, "shouldn't assume everyone will improve further with T4/3 @ 75% if they say they currently feel improved at 52% ", then please read my reply again and you will see that I neither inferred nor assumed such a thing ( and I haven't edited anything to that effect!) and I hope New2thyroid understands that
I used to make a list of all the things I wanted to raise at appointments and took that with me for reference....as I've said to others it stopped me quacking like a demented duck when I was anxious and trying to explain myself!!!
It's a bit of a slog isn't it, but you'll get there.
No i wasn't intending to be critical of your reply or approach .. which i always find considered and helpful.I think it was just the '50mcg' that made me raise an eye brow . perhaps i should have checked if that's what you meant, before writing you an essay .. sorry DD
x Got out of bed with a bee in my bonnet this morning.
And yes your probably right , without the T3 the Levo might well need increasing at some point, an awful lot of us need a little bit more than 100mmcg .
I think I probably got out of the bed on the wrong side.... bugs on the rampage today so a tad crosspatch!!I understand why you picked up on the 50mcg....I added an edit.
That was my careless mistake.....you were correct to point it out.
I started taking thyroxine in 1973 and was told in 1980 that I would get osteoporosis and heart problems later in life if tsh was kept suppressed. don’t understand how they knew this as thyroxine had only been used for 5 years. I have been suppressed for 49 years and still waiting for it!
Mines been mostly around 0.04 /0.05 level , sometimes 0.02 , for about 20yrs. (i'm aged 55 now )I've been told by my GP 'you'll die ! ' (if you don't reduce to 100mcg ,i currently take 112mcg , and have been on 150mcg in the past)
Still waiting for 'death' .... but then he didn't tell me what i was supposed to be dying of ,so how will i know ?
... and have had absolutely no heart issues or bone issues at all .
Likewise except 0.01 to 0.02 for nearly 50 years, I am 70. Unknowlegable doctors yo yod with my dose for 40 years quoting tsh and I missed a lot of years feeling poorly. I now try not to visit doctors and keep my dose stable where I feel healthy. Blow the tsh!
I believe it takes a very long time to recover the TSH after its been low for so long … I read that somewhere just can’t recall. Ive been on the same 100mcg levo and 10mcg T3 for 5 years always had a very low TSH and last year it has finally started to rise.
The TSH test is basically a useless test when you are taking a T3 alone or in a NDT or in addition to a T4 med. Most Dr.s do not understand this. Most Endo's are clueless!! Your T4 and most importantly your T3 are what you need to be concerned with. Good luck with a doctor that basically is looking at your TSH and prescribes accordingly. You had hair loss because your T3 was low. Your T3 should be in the 70% to 75% range. A T4 med WILL lower your TSH, but if you aren't properly converting that T4 med into the proper amount of T3, you will start to see all the symptoms that you had. You appear to have a conversion issue. I don't have any suggestion about how to convince your Endo of this. You may need to hunt around until you find a Dr. who knows what they're doing as far as the thyroid goes.
Hi, I have been in the same situation for years. I am sorry to say that your GP and your endo will jump up and down and say your taking to much Thyroxin simply because your TSH is suppressed. I think the NHS figure starts at around .5 so you are very mildly supressed in the eyes of the NHS. In my area, my thyriod blood test , they only test my TSH. Get the picture. Now why are you supressed. The most proable reason, is you have been taking some T3 , are you aware it can take up three months to get your TSH back to the level that the NHS will accept.?Here is a good example. My TSH was around .001 ie surpressed, and i was on 75MCR and 1/4 grain armour. But my bloods were almost identical to my dose of 100 MCR of T4. On T4 my tsh is .77 well with on range. Good luck as I feel your going to need it.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.


")