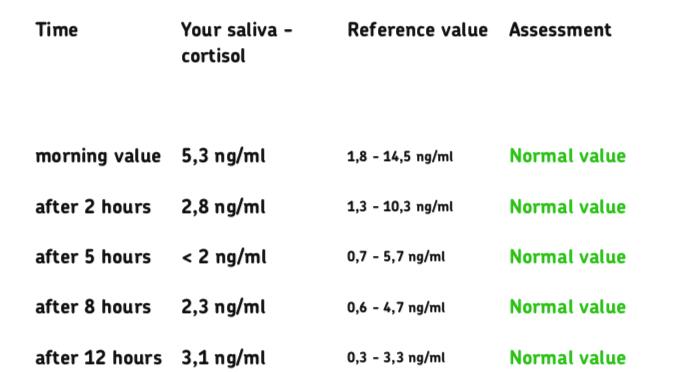
I did a saliva cortisol test as part of my investigations into my Hashimoto's, and although it came back saying my results were "normal", the curve of the graph wasn't. It should go down over the course of the day, not tick back up in the evening.
I'd love to hear your thoughts!
Written by
tealtortoise
To view profiles and participate in discussions please or .
• Morning at the top of the range - yours at 5.3 is only 28% through range should should be much higher, a good result would be around 14.
• Noon approximately 75% of the range
• Evening close to 50% of the range
As there's no time with your results I think the after 2 hours and after 5 hours will both be too low.
• Nighttime at the bottom of the range - the after 12 hours is probably the equivalent of this one and is at the top of the range, a level of 0.5ish to a maximum of 1 would be a good result.
I'm afraid I can't advise what to do, you need to raise the morning levels and lower the nighttime one but I don't know how you can do that.
Are you experiencing any symptoms? Certainly your cortisol levels are nor following the typical curve. Cortisol should be at the highest first thing in the morning & then drop as you say. Things that will elevate your cortisol are oestrogen contraceptive pill, HRT & biotin. Plus if you haven't rinsed your mouth prior to the test. Depending on what symptoms you may be experiencing, it might be worth chatting to your GP about it.
Thanks Pauline - I don't have really any symptoms apart from a tiredness some days, but I wouldn't call it ongoing fatigue. I do sometimes feel dizzy when I first stand up in the morning as well. I'm not on the pill or HRT, although there might be biotin in my B complex vitamin I take daily.
Your results are good compared to some on the forum and at least show adrenals are fully functioning and you stay within range.
Evening appears the most elevated. Do you fall asleep ok?
I would say adequate thyroid hormone, nutrients & iron, managed antibodies, supplementing Vitamin C and an evening yoga class would encourage a better circadian rhythm (curve).
Did you get DHEA tested at the same time? This would give an idea how advanced your adrenals struggle are.
What are your most recent thyroid levels and vitamin levels
Getting thyroid levels optimal should improve adrenals
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested. Also EXTREMELY important to test vitamin D, folate, ferritin and B12 at least annually
Low vitamin levels are extremely common, especially if you have autoimmune thyroid disease (Hashimoto's) diagnosed by raised Thyroid antibodies
Ask GP to test vitamin levels
Are you on strictly gluten free diet?
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
Last dose of Levothyroxine 24 hours prior to blood test. (taking delayed dose immediately after blood draw).
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
If/when also on T3, make sure to take last third or quarter of daily dose 8-12 hours prior to test, even if this means adjusting time or splitting of dose day before test
Is this how you do your tests?
Private tests are available as NHS currently rarely tests Ft3 or thyroid antibodies or all relevant vitamins
Thank you so much SlowDragon . I have had my levels tested recently and under those ideal test circumstances. My iron, folate, B12, and vitamin D are all normal. I have managed to get my vitamin D up from 58 to 133.
TPO antibodies > 1000, TG antibodies 34. 25mg of levothyroxine brought my TSH from 3.8 to 2.57 as of the last test.
I am just waiting for a coeliac test in a couple of weeks after which I will be going gluten free.
Thank you very much for all your recommendations. I normally just do Medichecks as my GP won't test vitamin levels or re-do my thyroid tests, but it gets pricey.
Standard starter dose of levothyroxine is 50mcg unless over 65 years old
Levothyroxine doesn’t top up failing thyroid, it replaces it. So it’s important to increase levothyroxine dose up as fast as tolerated
The aim of levothyroxine is to increase dose slowly upwards in 25mcg steps until TSH is ALWAYS under 2
Bloods should be retested 6-8 weeks after each dose change or brand change in levothyroxine
Typically, unless extremely petite most people will eventually need at least 100mcg levothyroxine per day
When adequately treated, TSH will often be well below one.
Most important results are ALWAYS Ft3 followed by Ft4. When adequately treated Ft4 is usually in top third of range and Ft3 at least 60% through range (regardless of how low TSH is)
Extremely important to have optimal vitamin levels too as this helps reduce symptoms and improve how levothyroxine works
Please add actual results and ranges on folate, ferritin and B12
Cheapest option for just testing TSH, Ft4 and Ft3 is Monitor My Health (NHS private testing) at £26.10 if order via Thyroid U.K. website (standard price £29 )
Even if we frequently don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or near full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
Thanks! My TSH was never high enough for my GP to agree to put me on a full dose. At its highest it was 3.8, and I think it needs to be over 5 for them to even think about medication.
I only managed to convince her to put me on 25mg because we're trying to conceive and optimal for TTC is < 2.5 TSH. I don't think she'd consider upping my dose unless my TSH got higher.
Utterly ludicrous. High thyroid antibodies confirms autoimmune thyroid disease
See thyroid specialist endocrinologist
Your under medicated
Have you had coeliac blood test done
Are you now on absolutely strictly gluten free diet?
Email Thyroid UK for list of recommend thyroid specialist endocrinologists...NHS and Private
tukadmin@thyroiduk.org
The aim of levothyroxine is to increase dose upwards in 25mcg steps until TSH is ALWAYS under 2
When adequately treated, TSH will often be well below one. Most important results are ALWAYS Ft3 followed by Ft4. When adequately treated Ft4 is usually in top third of range and Ft3 at least 60% through range (regardless of how low TSH is)
Extremely important to have optimal vitamin levels too as this helps reduce symptoms and improve how levothyroxine works
And obviously optimal vitamins essential for any pregnancy
TSH should be under 2 as an absolute maximum when on levothyroxine
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
New NHS England Liothyronine guidelines July 2019 clearly state on page 13 that TSH should be between 0.4-1.5 when OPTIMALLY treated with just Levothyroxine
Note that it says test should be in morning BEFORE taking levothyroxine
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
(That’s Ft3 at 58% minimum through range)
You can obtain a copy of the articles from Thyroid UK email print it and highlight question 6 to show your doctor
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.