Hi everyone. I’ve had some test results back. I had RAI in 2011 for hyperthyroidism and I’m therefore hypo. I’ve never really felt healthy since and in more recent years have got worse with aches and pains, anxiety, low energy levels, weight gain and more.
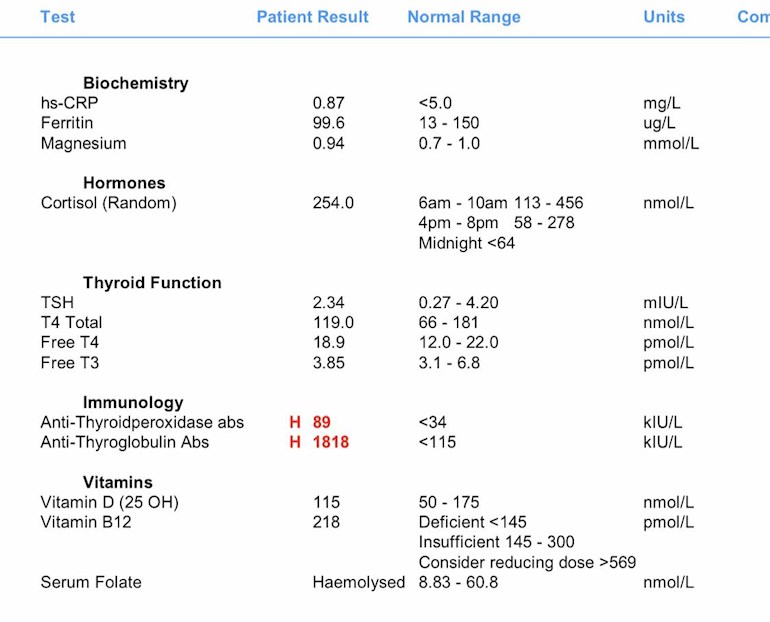
So as you can see, B12 is low so I know what to do there but the antibody results are out and I’m not sure what this means as I don’t have a thyroid anymore. Please could anyone help me on the antibodies tests?
My thyroid tests were ok although the free T3 seems on the low side so not sure if that’s optimal? My T3 was low on a previous test at the doctors and I’ve increased my levo since.
The serum result shows damaged red blood cells but there was a note saying this might be the way the test was taken and so best to test again.
Thanks in advance.
Written by
HypoFrog
To view profiles and participate in discussions please or .
Autoimmune hypothyroidism also called hashimotos usually starts with a hyper phase and then as it progresses there are periods of hypo and periods of hyper.
The antibody tests that nanaedake mentioned are the ones that test for graves.
The ones on your results I think suggest hashimotos but maybe someone will confirm this as I am not great on antibodies.
TPO and Tgab are more common in Hashimotos thyroiditis but can sometimes be found in Graves disease. I understood that normally TPO antibodies disappear when the Thyroid is eventually completely destroyed by Hashimotos disease. I would think there needs to be some thyroid tissue in order to activate TPO antibodies so perhaps this is the case for you?
Email Dionne at Thyroid UK for list of recommend thyroid specialist endocrinologists who will prescribe T3
tukadmin@thyroiduk.org
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
You can obtain a copy of the articles from Thyroid UK email print it and highlight question 6 to show your doctor please email Dionne at
tukadmin@thyroiduk.org
Professor Toft recent article saying, T3 may be necessary for many, note especially his comments on current inadequate treatment following RAI
Even if we don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until on full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
A small Dutch double-blind cross-over study (ArchIntMed 2010;170:1996) demonstrated that night time rather than morning dosing improved TSH suppression and free T4 measurements, but made no difference to subjective wellbeing. It is reasonable to take levothyroxine at night rather than in the morning, especially for individuals who do not eat late at night.
Sorry to say that your ft3 at 3.85 is not normal far from it and is the reason you feel so bad you should be trying for at least 6.0 This could be due to low magnesium levels affecting the conversion from t4 to t3 . You do not say if you are taking magnesium supplements
Your magnesium test indicate a good level of magnesium but this is only in the blood most of the magnesium is stored in the bodies cells in the Mitochondria so cell levels could be low and blood levels normal so taking magnesium glycinate or magnesium chloride oil might work if your not taking magnesium supplements at the moment.
Otherwise you need to start taking t3 as well or change your medication to NDT
Natural Desiccated Thyroid which contains both t4 and t3 and calcitonin
Your TSH is also high at 2.34 aim for a value of 1.0
Almost everyone in the west is deficient in magnesium if not supplementing due to poor diet/ food
You say you had RAI treatment this is normally given to patients with thyroid cancer after the thyroid has been removed but you do not really mention having cancer you did mention not having a thyroid though
The NDT might be the best option as this contains calcitonin which is important for bone health normally produced by the thyroid
The NHS does not provide this any more so you might need to go private or you could make a case to the NHS as a special need as a Named Patient to obtain it from the NHS for free
Thank you. I had RAI due to Hyperthyroidism, perhaps graves but I don’t recall. I had the option of surgery or RAI but as a singer, I didn’t want to risk damage to the vocal chords so opted for RAI.
I wasn’t really informed much at the time. I thought they’d removed the whole thyroid but perhaps not.
Looking back, there’s so much I should’ve known more about but I just didn’t know at the time about the complications. ☹️
They can’t remove the entire thyroid and you had RAI you would think that would have taken care of any remnants, I would be very concerned about the high Antibodies and see Endo sooner than later.
Im thyroid-less (cancer) no thyroid is no joke its life sucking.
I too had RAI back in 2005 and given a diagnosis of Graves and after a period of about 15 months on anti thyroid medication this is the first treatment offered by the NHS as otherwise they offer a thyroidectomy. I was well on the AT medication, but I wasn't offered the option of staying on a low dose anti thyroid medication long term, which now, with hindsight believe this to be an option we should all be given.
Hyperthyroidism can be caused by Graves Disease so maybe this was your diagnosis.
RAI is slow burn and eventually burns out your thyroid in situ, rendering it disabled and you with hypothyroidism.
T4 - Levothyroxine is a storage hormone and your body needs to be able to covert this hormone into T3 which is the active hormone that the body runs on and is is said to be about 4 times more powerful than T4. There is room for you to have an increase in Levothyroxine which in turn should improve your T3 status as it is low T3 that gives you symptoms you are currently dealing with and this will also lower your TSH as most of us feel better with this number being around 1 or under.
Your ability to convert the T4 into T3 can be compromised if your vitamins and minerals are not maintained at optimal levels and read after RAI vitamins and minerals can be trashed and that primary hypothyroidism caused by RAI more " challenging to treat " .
It is essential that you are dosed and monitored on T3 and T4 blood tests with the aim being that they a both in upper quadrant of their relevant ranges and balanced, with most people feeling well when the T3/T4 ratio when on Levothyroxine is around 1/ 3.5 - 4.5 : T3 to T4 : with most people preferring a 1/4 or lower : T3 is said to be about 4 times stronger than T4 so you current conversion ratio is coming in at 4.91 :
The thyroid is major gland responsible for full body synchronisation, including your physical, mental, emotional, psychological and spiritual wellbeing, your inner central heating system and your metabolism.
A fully functioning working thyroid would be supporting you on a daily basis with approximately 100 T4 + 10 T3 and I personally think if there has been a medical intervention either surgery or RAI that both these vital hormones should be on the patient's prescription for if, and probably when they will be required.
Some people can get by on T4 alone: some people simply stop converting for some reason at some point in time : and some people simply need both these essential hormones dosed and monitored independently to bring both T3 and T4 into balance and to a level of wellness acceptable to the patient.
You might like to read a book written by a doctor who has hypothyroidism : Barry Durrant-Peatfield writes in an easy understand manner and I found his book Your Thyroid and How To Keep It healthy - invaluable :
If you do find out you have Graves Disease the Elaine Moore Graves Disease Foundation website is well worth dipping into as Graves is an autoimmune disease and as such it's for life, and you may find reading around this poorly understood and badly treated AI disease of help.
After RAI I developed thyroid eye disease, so now manage lingering Graves, TED and hypothyroidism becoming very unwell about 8 years after RAI treatment. I am now self medicating and buying my own full spectrum thyroid hormone replacement and much improved and have my life back after the NHS refused me a trial of T3 back in early 2018.
My cognitive functions were severely compromised and I took to writing out what I thought I needed to remember and underlining and rereading information several times over.
If I read out loud to myself I found it resonated a bit better.
I'm dyslexic as well - so it was a mountain and half - but you can do it :
Just start by reading the posts on here, stuff does sink in, trust me.
Yes Graves is an autoimmune disease - that just happens to attack the thyroid and it is because the thyroid is such a major organ the symptoms experienced can be diverse with some considered life threatening.
Yes some people have both sets of antibodies - and Hashimoto's initially presents in the same way but isn't treated with any anti thyroid drugs, like Carbimazole and isn't treated with RAI.
With Hashimoto's you are dosed with T4 - Levothyroxine and your thyroid the victim of smaller bursts of antibodies over a period of years and with every attack your thyroid becomes a little more disabled. These attacks can be referred to as hyper swings and then followed by a period of recovery but with a gland bit more less able than before the attack, which results in constant adjustments to medication levels as the gland eventually dies and you become fully hypothyroid.
Your TSH is too high and think you would feel better with it down below 1 and you have room for a dose increase of T4 - Levothyroxine.
Your conversion isn't optimal, a dose increase might do it - but there's no guarantee - I increased my T4 to over the range just to see if I felt any better but it caused me bad headaches and further anxiety.
T3 - Liothyronine was like a light bulb moment for me, my brain switched on again, and the heaviness of my head lifted, and I woke up relaxed and at peace with the world - and I know that probably sounds corny but it's true.
I tried a T3/T4 combo and that worked for me and then I tried NDT and that also worked. At the time NDT was easier to buy and I do feel less turbo charged as since I haven't a thyroid believe the full spectrum thyroid hormone replacement more appropriate, replacing like with like.
I don't know the answer re Hashimoto's :- you'll have to adjust meds on occasion as the thyroid dies : NDT is 1 tablet to adjust : T3/T4 combo generally 2 tablets that need to be balanced : sadly it's all trial and error and comes down to your personal preference :
Can I please suggest that you update the forum members by starting a new post with these results and ranges.
Not many seasoned members look back two days, let alone a month, at old posts as it gets too confusing reading through everything all over again.
Just give a brief history and I'm sure you'll get more replies than way down here.
I remember answering you so took a look, but you need more opinion than me so take full advantage of the many and start a new post for old and new eyes to take a look.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.