I am currently taking 100mcg of levothyroxine. I was also thinking about self medicating with 5mcg of liothyronine. Can anyone help me interpret my blood work.
Thanks
I am currently taking 100mcg of levothyroxine. I was also thinking about self medicating with 5mcg of liothyronine. Can anyone help me interpret my blood work.
Thanks

Marcus36271
Most people wont know the reference ranges for these Medichecks results so for more members to comment you might want to resubmit your picture and show the ranges.
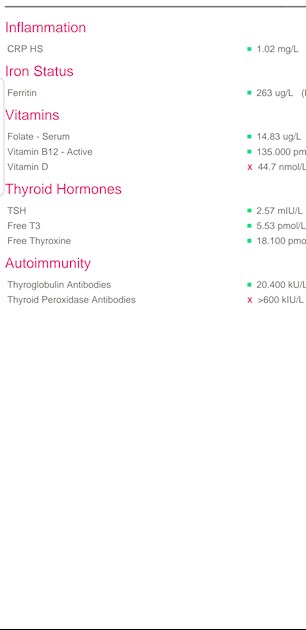
However, as you're on 100mcg Levo, straight away it's obvious that you are undermedicated. When on Levo only, the aim of a treated hypo patient generally is for TSH to be 1 or lower with FT4 and FT3 in the upper part of their ranges if that is where you feel well.
Your FT4 at 18.1 (12-22) is 61% through it's range. Your FT3 at 5.53 (3.1-6.8) is 66% through range. They are well balanced, again showing that it's Levo you need to increase. You don't need the addition of T3.
Ask your GP for a 25mcg increase in Levo and use the following information to support your request:
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3. You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
Also, NHS Leeds Teaching Hospital
has this on their website:
pathology.leedsth.nhs.uk/pa...
Thyroxine Replacement Therapy in Primary Hypothyroidism
TSH Level .......... This Indicates
0.2 - 2.0 miu/L .......... Sufficient Replacement
> 2.0 miu/L .......... Likely under Replacement
**
Your TPO antibodies are well over range which confirms that you are positive for autoimmune thyroid disease aka Hashimoto's which is where the thyroid is attacked and gradually destroyed. Fluctuations in symptoms and test results is common with Hashi's. Did you know you have Hashi's? Most doctors dismiss antibodies as being of no importance and know little or nothing about Hashi's and how it affects the patient, test results and symptoms. You need to read, learn, understand and help yourself where Hashi's is concerned.
You can possibly help reduce the antibodies by adopting a strict gluten free diet which has helped many members here.
Gluten contains gliadin (a protein) which is thought to trigger autoimmune attacks so eliminating gluten can help reduce these attacks.
You don't need to be gluten sensitive or have Coeliac disease for a gluten free diet to help.
Gluten/thyroid connection: chriskresser.com/the-gluten...
stopthethyroidmadness.com/h...
stopthethyroidmadness.com/h...
hypothyroidmom.com/hashimot...
thyroiduk.org.uk/tuk/about_...
Supplementing with selenium l-selenomethionine 200mcg daily can also help reduce the antibodies, as can keeping TSH suppressed.
**
Hashi's and gut absorption problems tend to go hand in hand and can very often result in low nutrient levels or deficiencies. Yours aren't too bad but:
Vit D: 44.7nmol/L = 17.88ng/ml
This is in the Insufficient category rather than Deficient, maybe not low enough for your GP to prescribe a supplement.
The Vit D Council recommends a level of 125nmol/L (50ng/ml) and the Vit D Society recommends a level of 100-150nmol/L (40-60ng/ml). For your current level, the Vit D Council suggests supplementing with 4,900iu D3 daily, nearest is 5,000iu.
Retest in 3 months.
When you have reached the recommended level then you'll need a maintenance dose to keep it there, which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. You can do this with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
there are important cofactors needed when taking D3 as recommended by the Vit D Council -
vitamindcouncil.org/about-v...
D3 aids absorption of calcium from food and K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking tablets/capsules/softgels, no necessity if using an oral spray
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking tablets/capsules, no necessity if using topical forms of magnesium.
naturalnews.com/046401_magn...
Check out the other cofactors too (some of which can be obtained from food).
**
Active B12, folate and ferritin seem to be OK, although I can't remember Medicheck's range for folate. If there is a proper range with an upper and lower limit, then folate should be at least half way through the range.
Hi Susie
Thank you kindly for your in depth reply. Will asked gp for 25mcg extra levothyroxine. Fingers crossed
Good luck. Your GP may need educating, take as much evidence as you can ")