I was diagnosed in December and have been taking 50 mg Levothyronxine. Still no change in the symptoms - low mood, no energy, weight gain, dry skin and so on .
A big thank you to the people who suggested that I get a more detailed blood test - tho' I had to cause a bit a rumpus at the Doctors. Yes I have Hashimoto and are now starting no GF diet. I have low vitamin D and have bought some over the counter vitamins and have been started taking 50 ug per day.
Doctors suggesting I increase to 75mg Levothyronxine and will be getting a prescription next week. I yet to have a face to face consultation with the doctors as they now do telephone consultations. I feel that the medics are reluctant on all levels either to send me to a specialist or prescribe a different medication.
All comments valued!!
Written by
soundeditor
To view profiles and participate in discussions please or .
At this stage there is really no need to send you to a specialist. Hashi's has been confirmed on your results sheet, there is no specific treatment for that, it's the resulting hypothyroidism that is treated and you are on Levo. Often we are best being treated by our GPs, most endos are diabetes specialists and know very little about the thyroid, and where Hashi's is concerned they seem to understand it even less and can really mess about with changing doses.
Also, there's no need to prescribe a different medication. What are you thinking of? There's nothing for the Hashi's other than helping yourself, which you are doing with a gluten free diet. Also you can supplement with selenium l-selenomethionine 200mcg daily can also help reduce the antibodies. If you are thinking of a different thyroid medication, your GP can only prescribe Levo. The NHS doesn't prescribe Natural Desiccated Thyroid and only an endo can prescribe T3 but at the moment they're being told not to give it to new patients. But you may not even need T3. You've been on Levo for 2 months, a very short time, so you need to give it a chance to work. It can take many months for us to feel well after diagnosis.
Accept the increase in Levo, make sure that you are retested 6-8 weeks later, then another increase if necessary. Retesting/increasing should continue until your levels are where they need to be for you to feel well. The aim of a treated hypo patient generally is for TSH to be 1 or below or wherever it needs to be for FT4 and FT3 to be in the upper part of their respective reference ranges when on Levo, if that is where you feel well.
When booking thyroid tests, always book the very first appointment of the morning, fast overnight (water allowed) and leave off Levo for 24 hours. This gives the highest possible TSH which is needed when looking for an increase in dose or to avoid a reduction. TSH is highest early morning and lowers throughout the day. It also lowers after eating. This is a patient to patient tip which we don't discuss with doctors or phlebotomists.
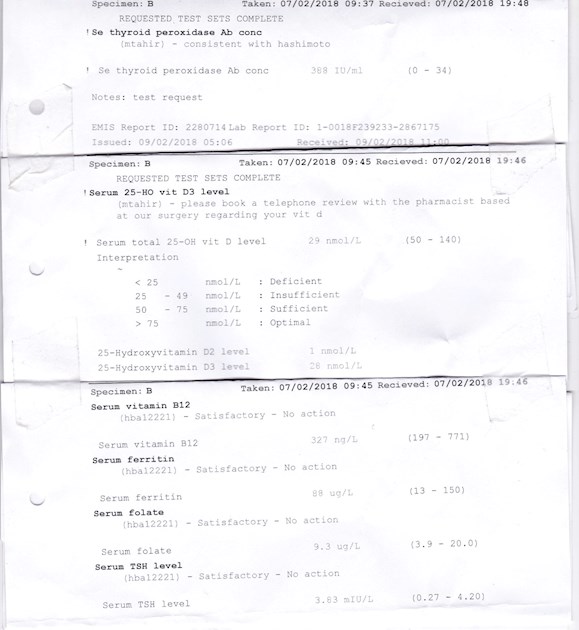
As far as your Vit D is concerned, 50mcg D3 = 2000iu. That's not enough to raise your level of 29nmol/L to the level recommended by the Vit D Council which is 100-150nmol/L. The NICE Clinical Knowledge Summary suggests for levels below 30 then loading doses should be prescribed - see NICE treatment summary for Vit D deficiency:
"Treat for Vitamin D deficiency if serum 25-hydroxyvitamin D (25[OH]D) levels are less than 30 nmol/L.
For the treatment of vitamin D deficiency, the recommended treatment is based on fixed loading doses of vitamin D (up to a total of about 300,000 international units [IU] given either as weekly or daily split doses, followed by lifelong maintenace treatment of about 800 IU a day. Higher doses of up to 2000IU a day, occasionally up to 4000 IU a day, may be used for certain groups of people, for example those with malabsorption disorders. Several treatment regims are available, including 50,000 IU once a week for 6 weeks (300,000 IU in total), 20,000 IU twice a week for 7 weeks (280,000 IU in total), or 4000 IU daily for 10 weeks (280,000 IU in total)."
Each Health Authority has their own guidelines but they will be very similar. You could go and see your GP and ask that he treats you according to the local guidelines or this summary and prescribes the loading doses. Once these have been completed you will need a reduced amount (more than 800iu so post your new result at the time for members to suggest a dose) to bring your level up to what's recommended by the Vit D Council - which is 100-150nmol/L - and then you'll need a maintenance dose which may be 2000iu daily, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. You can do this with a private fingerprick blood spot test with City Assays vitamindtest.org.uk/
If you don't get the loading doses then you should roughly follow the suggestions in the Summary and I would start off with 10,000iu daily for 4 weeks (total 280,000iu) then reduce to 5000iu daily and retest a couple of months after starting.
Your doctor wont know, because they are not taught nutrition, but there are important cofactors needed when taking D3
D3 aids absorption of calcium from food and K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds.
Magnesium helps D3 to work and comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds
As for your B12, it's on the low side. An extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
You could supplement with sublingual methycobalamin 1000iu and to balance all the B vitamins also take a good B Complex.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.