My gastric ulcer is now healed and I've been supplementing, including B12. I waited a month after stopping the PPI (to heal the ulcer) and then had a blood test done.
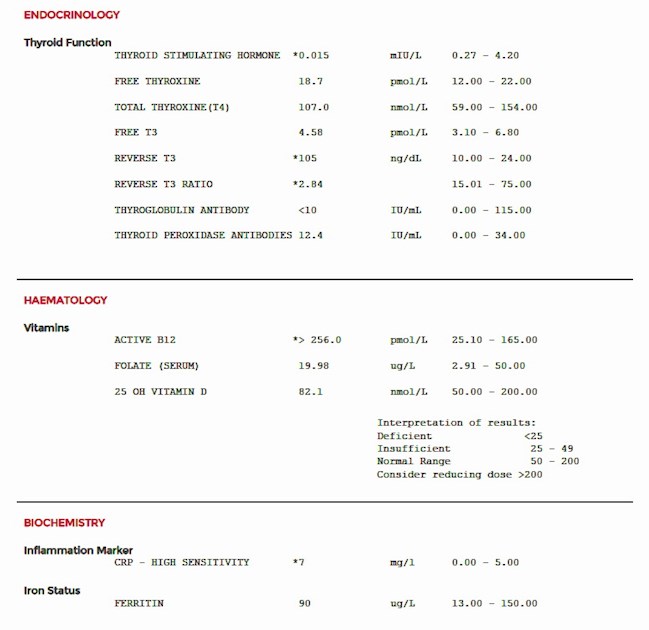
Results are attached. This is the first time I've had Reverse T3 tested and I'm seeing my GP next week to discuss the results, as I think its time I was referred to an Endo, something my GP has previously refused to do. It looks like I'm not converting, so any advice or suggestions will be very appreciated.
My CRP has come down since August, when it was 19 and I had the ulcer, I'm not sure why it's still above range and I'm not aware of any infection.
Many thanks.


")