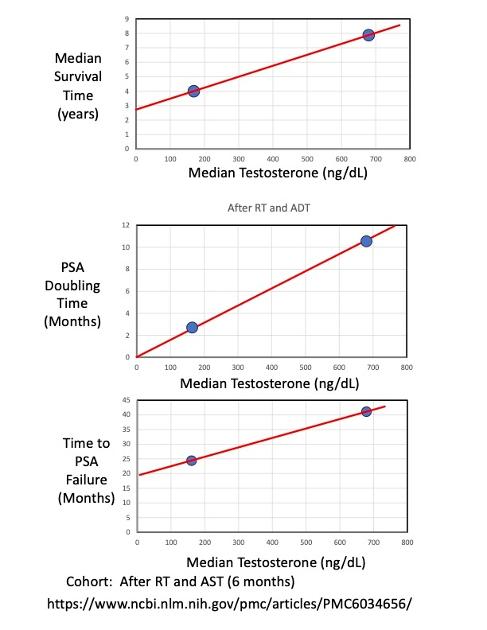
These companion plots compare: (A) median survival times, (B) PSA doubling times, and (C) Time to PSA Failure for two different levels of testosterone: Low and Normal. The low testosterone has a median value of 162 ng/dL [120-236] and the average normal T = 680 ng/dL. The cohort is 58 men with unfavorable intermediate risk who underwent RT and 6-months of ADT.
Low testosterone after completing ADT is associated with (A) about 1/2 of the median survival time; (B) a much shorter doubling time (factor of 3.8 X shorter); and (C) a much shorter time to PSA failure.
In other words, men who had normal Testosterone after completing ADT lived twice a long as men who had low testosterone after ADT.
Shorter doubling times are associated with more aggressive PCa, as supported by the much shorter time to PSA failure.
The important takeaway is that having a low testosterone (T < 280 ng/dL) after completing ADT is associated with extremely poor survival outcomes.
One thing men in this situation can do is supplement their Post-ADT testosterone to get it back to normal levels as quickly as possible. It can double your lifetime !
It is interesting that the plot of PSA doubling time plot exactly goes through the origin (0,0) when extrapolating the two data points by only a short distance. I'm sure some MD could explain why this is.
Have you yet asked a qualified PCa Doc why your proposed protocols are not standard care.....providing miraculous results for a great many men? There are those who have dedicated their lives to PCa research, but they have missed this??????
I'm guessing big Pharma has had a role to play here...
But, to debate your point, oral estrogen (DES) was the Standard of Care for over 20 years , from 1960's-1980's, because it was the only drug available that chemically castrated men. It was eventually dropped when Lupron was invented because of blood clots at high-doses of DES (5 mg/day). Later, the dose was reduced to 1 mg/day, with had fewer side effects.
Huggins won the Nobel Prize in 1966 for his discovery that estrogen chemically castrated men. Most docs today have forgotten, or likely never learned, the important (and relevant) history of estrogen use.
There is published data (6-year survival probability) for oral estrogen that shows no difference in outcomes comparing Estrogen to Lupron ADT. This makes sense, because estrogen and Lupron have exactly the same mechanism of action (suppression of LH and FSH hormones).
I'm currently editing a draft paper by Prof. Wassersug that reviews the history of estrogen use. It's very well written, with lots of references. He hopes to publish it soon.
Modern transdermal delivery of estrogen (TDE, via patches or gels) eliminates the previous problems with blood clots because it bypasses the liver. (Oral estrogen goes through the liver). Consequently, modern TDE has been recently found to have no bad cardiovascular side effects.
The reason TDE is not "approved" today is because there are no modern data on the 5- and 10-year survival outcomes. The TDE PATCH study, which has been going on for 10 years now, will publish their 5 & 10 year survival outcome data this Fall. That's how long it takes to approve things in the PCa world.
Are there also studies on the benefits of Dutasteride for improving survival....lowering the DHT? If high dosage didn't cause troublesome SEs, you could dispense with Lupron, etc and just do Dutasteride?????
I’ve continued to research the use of Dutasteride for treating PCa, and I found three different studies that reported the % reduction in Prostate Cancer Risk (there are more, also):
Study # of men % Risk Reduction
ARIA (2004) 4325 51 %
REDUCE (2010) 8231 23 %
combAT (2011) 4844 40 %
The average of these three studies is a 38% reduction in the risk of getting prostate cancer.
I don't know of any long-term studies of Dutasteride monotherapy, but I can check. It may be a good thing to try, in addition to ADT and RT.
Here's my PSA time history, showing the effect of starting Dustasteride. My PSA dropped by 70% after 3 months on Dutasteride, and no ADT. My T level is high 1060 ng/dL, because I supplement T (I have hypogonadism). I plan to stop TRT when I start my treatment plan, in case Dutasteride isn't sufficient.
A study published in 2012 European Association of Urology showed significant advantage to using Dutasteride ,around 60 % relative risk reduction for patients . (edit)
" Objective: To assess the effect of dutasteride on progression of PCa in patients with biochemical failure after radical therapy." " Dutasteride significantly delayed the time to PSA doubling compared with placebo after 24 mo of treatment (p<0.001); the relative risk (RR) reduction was 66.1% (95% confidence interval [CI], 50.35-76.90) for the overall study period. Dutasteride also significantly delayed disease progression (which included PSA- and non-PSA-related outcomes) compared with placebo (p<0.001); the overall RR reduction in favour of dutasteride was 59% (95% CI, 32.53-"
THANK YOU for posting this article! I had not seen it.
My PSA has gone down from 10 to 3.3 over 3 months on Dutasteride (0.5 mg/day). I will measure it again in a few weeks; I expect it to be lower, around 1-2.
I may have missed something as not read the paper yet but seems obvious that low T for an extended time will increase mortality as it is implicated in a whole range of proceses. But is the time from cessation of ADT to recovery a factor or just the ultimate level it reaches.
This is relevant for those of us in longer than 6 months who are high rusk so 18,24 and 36 months.
Good question. Unfortunately, I don't have data for ADT durations longer than 6 months.
I have plotted data on T-recovery vs time for a range of different ADT durations, from 3 up to 36 months. See attached plot.
If I had been on ADT for many years, I would want to do T-supplementation as soon as possible to get back to normal T-levels. Morgentaler's papers say that this is a safe thing to do.
I know about the estrogen stuff....wish we had the Patch results!!!
So, lfetime ADT for recurrent/metastasized men is a death sentence independent of death from PCa???? That seems to be the implication of some of what you have presented? You showed the incredibly high mortality rates for men with low T after recurrence/PSA increase?
I'm not trying to imply anything. I'm simply presenting published data and describing it.
Unfortunately, there is no data associating the length of ADT duration (months) with mortality probability.
That said, there may, indeed, be such an association (as you propose). Someone needs to dig into the databases and look for data that supports (or refutes) your hypothesis.
The other data that I presented above (in my reply to SimMartin) combines 6 different data sources and shows that, on average (remember, each man is different), the longer the someone does ADT the slower the natural T-recovery time is, in general. So, in other words, at any given time after stopping ADT, men (on average) with longer ADT durations will have a lower % of T-recovery.
We know that some men will recover their baseline T faster (or slower) than others. There's probably a factor of 2-3 X scatter in the T-recovery times. That's typical for PCa data...very wide distributions with large amounts of scatter.
Other factors may affect the T-recovery time, too. Some of those men may have been hypogonadal or older, in which case their baseline T would likely be lower (compared to younger men with higher baseline levels of T). Physical fitness likely affects with baseline T, also.
For the PCSM mortality rate plot, the same factors could apply, as well. High baseline-T, high fitness level, and/or younger age might be correlated with lower mortality rates, and visa-versa. We just don't know, though, because there is no published data about these things.
You, of course, are welcome to make your own hypotheses and draw your own conclusions. You may be right, or you may be wrong. More data is needed.
The problem is that existence of a correlation/association does not imply a causation. Unfortunately, this makes it difficult to determine the best treatment plan at any stage in this complex process.
I would like to draw your attention to the first 2 years after PSA failure for PCSM. The probability of prostate cancer specific mortality (PCSM) is the same (i.e., zero) for both low-T and Normal-T during the first 2 years. The two curves don't really start to spread apart until more than about 3.5 years after PSA failure. So, there appears to be a window of time of about 3 years before bad things really start to happen when your T is low.
The important question is: should you supplement your T during this window of time? Morgentaler has published data that shows it's a safe thing to do (in the castrate-resistant regime after PSA Failure).
In summary, the effect of longer ADT durations on PCSM is simply unknown. One could speculate that the separation between the two curves ( Low-T and Normal-T ) might stay the same, spread apart, or become closer as ADT duration increases. More data is needed.
The study looks into the short term 6 months or less vs long term +2 years with a combination of radiotherapy. LHRH was used for the ADT.
CONCLUSIONS
The combination of radiotherapy plus 6 months of androgen suppression provides inferior survival as compared with radiotherapy plus 3 years of androgen suppression in the treatment of locally advanced prostate cancer. (ClinicalTrials.gov number, NCT00003026.
Thank you for the reference. I agree with its findings.
I think it's important, however, to make a distinction between the two different groups of men: (A) castrate-sensitive, and (B) castrate-resistant.
The study you reference is most likely for group (A), castrate-sensitive men. This is true because longer durations of ADT gives better outcomes. Only castrate-sensitive men have this kind of a response. For this group, lowering testosterone to near zero gives the best outcomes.
However, as PCa progresses, the opposite appears to be true for men in Group (B) (castrate-resistant). By definition, men in that group do not respond to ADT anymore, whether it is short duration or long duration. It just doesn't work anymore.
The plots I showed above support the hypothesis that higher testosterone gives improved survival outcomes for castrate-resistant men in group (B). This has been studied extensively, and reported by respected doctors, including Abe Morgentaler of Harvard.
The successful BAT therapy from Sam Denmeade at Johns Hopkins is an extension of this theory, which uses periodic super-high testosterone levels to "reset" the cancer cells to be sensitive to ADT again.
As far as I know, there is a lot of data to show benefit of longer duration of ADT, up to a limit, for RT + ADT. Tere is also data to show benefit of longer duration for metastatic men. Not sure why you say none/insufficient data?
I'm not aware of data showing a benefit of longer ADT for metastatic men, but it makes sense.
For someone on long durations of ADT (2-3 years), they likely have experienced both phases of PCa, namely: a first period of castrate-sensitivity, followed by a second period of castrate-resistance.
It is well-known that increasing the duration of ADT helps prolong the length of the first period when the patient is still castrate-sensitive. No question about that. More ADT is better while still castrate-sensitive.
However, I've not seen any data that longer periods of ADT help prolong the length of the second period (castrate-resistant). It probably doesn't help, because (by definition) being castrate-resistant means that ADT no longer works at any duration.
The survival times for metastatic men probably include contributions from both the first and second periods of time. That's my assumption when people report survival data (Kaplan-Meier plots). So, it makes sense that increasing the length of the first period (by increasing the duration of ADT) will also increase the total survival time for metastatic.
I assume that metastasis can likely occur anytime during the first or second period, (when treatment is unsuccessful).
What is unclear to me is how, or when, the occurrence of metastasis is related to the transition from castrate-sensitive to castrate-resistant. I suppose it's possible (and I'm guessing here) that metastasis occurs when a patient transitions from being castrate-sensitive to castrate-resistant (but that's just an unconfirmed theory). Personally, I think that hypothesis is untrue.
I'm sure, however, that there is a relationship between ADT duration and the time at which PSA Failure occurs (i.e., the time when a man transitions from being castrate-sensitive to being castrate-resistant).
I would be interested in any papers that talk about this.
Re RT + ADT for high risk men, a very good consortium study of 10000 men found that the longer the ADT duration, the better the metastasis-free and lower the PCa -specific mortality results...unfortunately, did not result in longer overall survival, wich peaked at an ADT duration of 19 months . My urologist said " we have many more questions than we have answers" He has an ivy-league MD, but humble!!!
Google Zoarsky prostate cancer and you will probably find the study....2022 I think.
I'm not sure the complexities of cancer will yield to a purely numbers approach.
There are always trends that can be discovered and plotted. But, as someone said, "correlation doesn't not imply causation". That's why we should always use the word "association" instead of "causation" in this business.
I will look for Zoarsky's paper(s).
Everyone agrees that in the castrate-sensitive regime that longer durations of ADT improve outcomes compared to shorter durations of ADT. That is well-established.
The important question is: "Does doing ADT in the castrate-resistant regime help?"
I'm sorry.....I don't have all those plots you have done memorized or immediately available. Didn't one show better results when T was higher after recurrence following RT + ADT? So, generally for men who have such a recurrence, until proven otherwise, such men are considered ADT sensitive and are prescribed ADT...thus keeping T low after recurrence.
Just found this in my hundreds of PCa bookmarks!!!
Yes on the debate about metastatic men......haven't done much direct research on that question, and I think I'll wait until I'm metastatic. I guess Bat is effective for some such men, and it does use cyclic ADT. I do think, but memory may be failing?, that ADT generally continued after initial ADT "fails".......a guru here has said basic ADT is continued because it is still working for some PCa variants, so keeps the total PCa load lower than it woulf be if basic ADT discontinued after "failure". Makes some sense to me!!!
We have more questions than we have answers ...very complex . Billions spent on research.
It's easy to put men into two distinct categories, (castrate-sensitive or castrate-resistant). However, there is likely a transition period during which there may be a combination of both states. Perhaps new PCa cells are castrate-sensitive and old PCa cells are the ones that become castrate-resistant?
I wish there was a blood test that could tell if you are castrate-sensitive or castrate-resistant. That would be cool !
As far as I know, the PSA test is used for that....imperfect it may be.
Yes, it makes great sense that there is a mixture of castrate sensitive and castrate resisistant mutations....thus the continuation of ADT even for "resistant" men. AT some point, one would guss all sensitive mutations are long gone...at which point ADT is totally useless, just bad SEs.
So, we agree that there is likely a transition period between 100% castrate-sensitive and then 100% castrate-resistant. I wonder how long that period is?
That would be a good question for Dr. Sam Denmeade at Johns Hopkins, who invented the BAT protocol.
I suppose if 100% castrate resistant, the theoretical benefit of BAT would be reduced???? I'd doubt there are any conclusive studies on % castrate sensitive. Idea for such a study, and what would the results mean....other than to determine a point at which there might be zero reason to continue ADT?
I agree, that we need a study to determine the optimum time to stop ADT, in terms of castrate-sensitive vs castrate-resistant status. Maybe Tall_Allen has some ideas about this?
I'm not an expert on BAT, but my understanding is that it works best on castrate-resistant men. I don't think it would work at all for castrate-sensitive men.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.