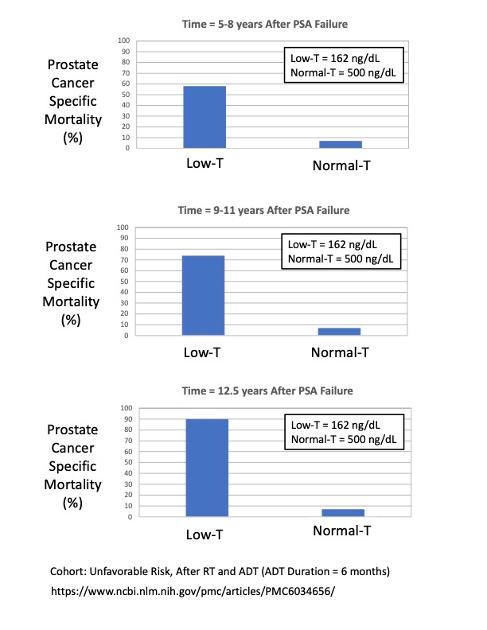
Here are comparisons of the Prostate Cancer Specific Mortality (PCSM) probability (%) for two different testosterone levels (Low-T and Normal-T)and three different Times After PSA Failure from Atkins (2018).
he median testosterone for the Low-T group is T = 162 ng/dL [120-236], and I assumed an average value of 500 ng/dL for the Normal group. The cohort is: Unfavorable Risk after TR and 6 months of ADT.
These plots show that the probability of dying from prostate cancer (after PSA failure) is significantly worse for men with Low-T. Since this data is after PSA failure, we can assume that the men in this cohort are castrate-resistant.
These data supports the statement that after PSA failure, in castrate-resistant men, a higher level of T is associated with significantly lower probability of death due to prostate cancer.
Written by
janebob99
To view profiles and participate in discussions please or .
You can get most of it on our bio. My husband did 9 months of iADT almost immediately after a radical prostatectomy because his PSA never went to 0 and he had positive nodes. He’s been followed for 23 years now and only went back on ADT a few years ago. I don’t imagine him going back off. The Oncologist says that the ADT is discouraging the proliferation of any prostate cancer cells that are not yet castrate resistant.
The reason I found the article interesting is that for 19-20ish years, he had a normal testosterone level and he’s still alive.
The fact that he's still alive after 20 years while having a normal T is wonderful!
It is also consistent with Morgentaler's Saturation Model, and papers that he was written, that show the prostate cancer growth rate (# of new cancer cells/day) is independent of testosterone level for T > 250 ng/dL. In other words, the PCa growth rate is saturated and does not increase for T levels in-between 250 and 1000 (or more) ng/dL. Note, however, there still can be PCa growing at a fixed rate in this T range....but, having a normal T doesn't make it any worse.
This is for men who had RT +ADT, correct? Then , recurrence is defined as nadir +2, correct? Isn't it possible that the mortality for low T men reflected not the T level but the aggressiveness of the PCa for those men, thus they continued ADT for longer after recurrence, whereas the High T men , even though official definition of recurrent was met, didn't otherwise have signs of very aggressive cancer and were not subjected to the longer treatment with ADT...thus the high T relative to the low T aggressive group?
Good question, but upon castrate resistance don't most docs immediately move onto more severe treatment while continuing ADT, not merely allow T to rise?
You are correct about most docs continuing to do ADT while on advanced treatment.
But, there's lots of evidence (see Morgentaller's papers and YouTube lectures), plus the paper I plotted above, that having a high T in the castrate-resistant regime is protective.
You may want to consider doing the BAT therapy protocol, which causes super-high levels of testosterone in a cyclic manner to "reset" your cells back to being castrate-sensitive. In the BAT protocol, you do continuous ADT, as well.
Yes, that's correct...all men had RT and then all men had 6 months of ADT in this cohort. Note, also, that all men had PSA recurrence/failure in this cohort at some (unknown) time during their progression.
I'm not following your theory very well, however. You speculate that "they continued ADT for longer after recurrence".
My first assumption is that the men started doing ADT at the same time when they did radiation treatment. My second assumption is that they experienced their PSA Failure after they had completed their 6 months of ADT. That's the most likely timeline of events.
There is no indication in this paper that some men did their 6 months of ADT after PSA Failure/recurrence. It's possible they did, but it's unlikely (and it wouldn't make sense).
The data I showed from this paper does not say, or imply, anything about whenPSA recurrence/failure occurred. The reported timeline is "Years following PSA Failure", meaning that time starts at 0 when each man had their PSA failure.
I do agree that the shorter lifetimes for low-T men reflects that their cancer was more aggressive than men with normal-T (in this cohort of Unfavorable Intermediate Risk men).
I think you could reasonably assume that all of these men in this cohort were castrate-resistant (because having reached PSA Recurrence/Failure (PSA > nadir + 2) is a primary definition of being castrate-resistant).
Many other papers report observations that higher levels of T is protective for castrate-resistant men. Morgentaler has published many papers supporting this observation. Successful results from the BATprotocol (periodic high-T supplementation) also support this observation.
So, in summary, I think that the PCSM mortality plots that I showed are in good agreement with many other published studies.
Unfortunately, no one knows why higher T is protective for castrate-resistent men. That's an open research question, I believe.
It seems to me that when chemical ADT was first introduced, there may be studies looking at its continuance post recurrence vs no ADT post recurrence. Has anyone seen such studies?
" Of the 227 patients who underwent post-prostatectomy RT, 95 (41.9%) received concurrent ADT for a median of 17.0 months. Despite more aggressive disease characteristics in the concurrent ADT group than in the RT-only group, the former had a better 5-year BCR-free survival rate than the latter (66.1 vs. 53.9%; p = 0.016), whereas the radiographic progression rate was not significantly different between two groups. On the other hand, salvage ADT after post-RT BCR significantly delayed radiographic progression (5-year radiographic progression-free survival; 75.2 vs. 44.5%; p = 0.002). "
Maybe later I'll look for a good meta-analysis.....one well-known Doc said those are the best for overall evidence of benefit, and that certainly is common sense if met-analysis is well done.
I find it hard to believe that probably 100,000 + men now living with recurrence are on ADT per their Docs' guidance , and there is no good proof of benefit, and the Docs do know the many negatives of ADT re SEs?
An RO told me...you can do ADT with your RT now, or you can do your ADT later !! He was suggesting RT for me would fail unless with ADT...in fact, much higgher probability of failure, but not a guarantee of failure from my understanding.....don't like it when I hear such things from Docs!!
"I find it hard to believe that probably 100,000 + men now living with recurrence are on ADT per their Docs' guidance , and there is no good proof of benefit, and the Docs do know the many negatives of ADT re SEs?"
Thanks for the reference, Kin (2018). And, thanks for bringing two new phrases to my attention, "Salvage ADT", and "Salvage ADT after BCR". I can now do a search on those phrases.
This paper by Kim (2018) supports the following conclusion:
" Doing ADT + RT after RP gives better outcomes than doing RT without ADT after RP."
That makes sense, because there can be castrate-sensitive micro-metatases outside of the prostate that are not identified by imaging.
You know...we are always looking for simple statements, such as: "Salvage ADT after biochemical occurrence (BCR) or PSA Failure is not effective because of castrate-resistance". But, this simple rule may be wrong...
It's possible that men who are nominally "castrate-resistant" still have some of their cancer cells that are still "castrate-sensitive". Perhaps there is a transition from being 100% castrate-sensitive, to being 50:50 sensitive and resistant, and finally to being 100% castrate-resistant. Meaning, that the transition from being fully castrate-sensitive to being fully castrate-resistant might occur over a significant period of time (i.e., a transition period, perhaps many months). If so, that could confound the data.
Regarding the paper by Kim (2018), I do want to call attention to one sentence in a paragraph from the paper that appears to be important:
"Supplementary ADT was classified into concurrent and salvage ADT according to time of administration. Concurrent ADT was defined as ADT administered before, concurrent with, or after RT. Salvage ADT was defined as ADT administered after a post-RT BCR. The ADT regimens were manipulated according to PSA response. When castration resistance occurred, further treatments, including cytotoxic chemotherapy, were initiated, based on the physician’s decision."
Is becoming "castrate-resistant" synonymous with "PSA Failure" or "Biochemical Recurrence, BCR")? I have always assumed that it is. If that is correct, then the sentence highlighted above indicates that chemotherapy was used after BCR had occurred. Doing that would confound the comparison of the data trends about salvage ADT in this paper
Of course, people who get chemotherapy after castrate resistance has occurred will do better than people who didn't get chemotherapy.
I will look for other papers that talk about salvage ADT.
Just my personal note. Be careful about losing your life to the research......I often feel that I have been unwise that way !! Maybe it is generally a much better use of the years we have remaining to search for the most trusted Docs available to you and mostly go with their guidance? Alternatively, go to Tall Allen's blogsite and read all that he has compiled there.....very comprehensive. Dives into multi-studies on many topics.
I could show you a recent MD video in which he questions the overall picture of cancer progression as generally understood by many Docs? Is he right......I don't know, but i suspect so. I didn't search for such a video...it found me!!! Yes, the micrometastases circulating in blood are part of his discussion!!
if I had your email, I'd forward something from Mark Storey RO...just popped up in my inbox. I suggest you Google Mark Storey MD RO and I think you'll find his website and link to his blog and all his musings.....many re PCa treatment. Based on what I have read.....were he easily accessible for me, He would be my RO!!!!!!
Thanks... said humbly, and maybe I'm wrong about self-doubt??? I do hope my suggestion re Tall Allen's blogsite is a good one.....and while not as study-oriented, Dr. Scholz videos are broad-ranging IMHO. PCRI.org I think.
and a personal marker for non-regional bone metastasis.....ALP test, which possibly could make one wonder if a negative PSMA PET scan is missing something ? SO far, thank goodness, aligns with my PSMA PET results.
All this is very stressfull, to say the least. But, the question is not "why me", rather "why not me? " 25% Americans diagnosed with cancer!!!
I appreciate our active dialog and your probing questions. It helps me to better understand how PCa behaves. (It's a sneaky bastard...).
I've read Tall_Allens websites quite a bit. He's an amazing collector and reporter of publications.
I'm doing something similar, except that I make graphs of the data and he doesn't. I'm experienced using Excel and PowerPoint because of my work (I'm a registered patent agent and have to make precise patent drawings). Before that, I worked as a Ph.D Nuclear Engineer for 20 years at Sandia National Laboratories doing magnetic fusion energy research).
I've read Mark Scholz's book. It's well written, easy to understand, and fun to read.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.