My goal is to find the minimum Bicalutamide dose that will keep my PSA relatively low until this 4th Covid wave passes and can proceed with my next treatment.
This post is a bit mathy, the bottom line of which is that the data summarized in the "Pharmacology of Bicalutamide" chapter of wikipedia were validated in my case. (en.wikipedia.org/wiki/Pharm...
Ground information before proceeding:
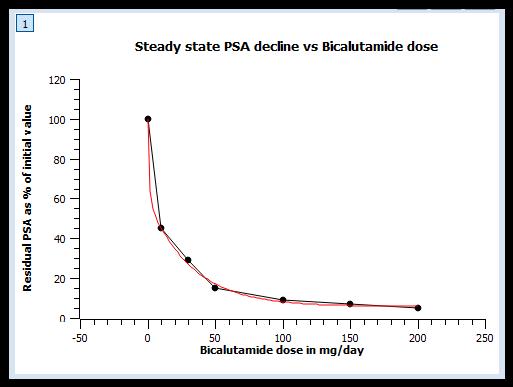
a) The reduction % of PSA, or alternatively the residual % after reduction, is dose related when the plasma steady state concentration has been reached.
b) Plasma steady state concentration is the condition where the daily/weekly Bicalutamide intake equates the elimination due to its decay in the blood. It goes without saying that the period for reaching steady state is related to Bicalutamide's half-life.
c) Interestingly enough, the plasma elimination half-life is dose dependent within the range of 5.6 to 7.5 days according to one study, or a uniform value of 5.8-5.9 days in others including a mention in a FDA registered document. This translates to 45 days (-2/+12) for reaching 99.5% of steady state for doses ranging from 5 to 80 mg/day. The following table was derived from the first study [180].
Dose / Half-life / 99.5% concentration
(mg/day) / (days) / (days)
5 / 7.4 / 56
10 / 6.4 /49
15 /5.8 / 44
20 / 7.3 / 55
30 / 7.5 / 57
50 / 6.0 / 46
80 / 5.6 / 43
d) The residual PSA (%) was approximated by a function, as in the graph on top, in order to make possible interpolation of in-between dose values.
My experiment until now:
1) Started at PSA 0.17 with 50 mg/day for 10 days. PSA went down to 0.09.
The equivalent steady-state dose from a concentration point of view was 27 mg/day, while that from the PSA decline point of view 5.0 mg/day.
2) Lowered the dose to 4x50 mg pills per week for the following 11 days and the PSA went down to 0.06.
The equivalent steady-state dose from a concentration point of view was 21.5 mg/day, while that from the PSA decline point of view 19.0 mg/day. Convergence between the two was noticed.
3) For the next 16 days I slashed the dose into half splitting two pills, i.e. 4x25 mg per week. The PSA remained at 0.06.
The equivalent steady-state dose from a concentration point of view was 20.0 mg/day, while that from the PSA decline point of view 19.5 mg/day. Convergence was strengthened further.
4) Next, will continue with the 4x25 mg/week dose to see how it goes. My current concentration is above the steady state equivalent of 14 mg/day dose, so PSA may rise. The interesting thing is what will be the doubling time of such a rise. There is this "huge" rounding error of 0.06 that can mask any upward or downward PSA undergoing movement. Will report here and then.
Written by
Justfor_
To view profiles and participate in discussions please or .
Nice work. I am trying to do the same with Xtandi. The maths indicate that standard 160mg dose is OK to build up to steady state - and logic suggests that steady state can be maintained thereafter by lower doses. But I am wondering if there is some resistance factor that should enter the equation which regulates the rate of uptake versus the existing saturation. Havnt found enough data to do this precisely yet.
My algorithm, implemented by the aid of an excel sheet, is to take on a day by day basis the sum of any newly added pharmaceutical quantity (for some days this may be null) and the already flowing within the plasma one and calculate one day's decay which it is carried over as the next day's initial condition. It is possible, like you suspect, that some resistance factor can build up with time, but this can be compensated by making the half-life shorter. There is no such data available that I know of. Only frequent PSA measurements can reveal if this is actually the case or not.
Here is the same, healthcare is ok with testing every 3 months, the rest are out of pocket, but not expensive (around 15 Euros). I use two labs in alternation, so to be able to spot any inconsistency.
You're lucky. Here in the U.S. I pay $6 for a monthly PSA test covered by my insurance, and for the 3 others I get each month I pay $38 for each. But $125 a month for weekly PSA testing doesn't seem bad. I can easily spend as much taking the wife to a nice dinner.
WOW - I never thought of that. I can now get a higher frequency of PSA test done locally - this will be interesting - thanks for the input - and happy Christmas
Update: 34 days later my PSA declined to 0.04 from 0.06.
It was a bit of a pleasant surprise as my self-derived model predicted a 0.06 -0.07.
That because by gradually reducing the weekly dose I am approaching the steady state Bicalutamide concentration from above, hence declining. The model estimates the residual PSA from the current (declining) concentration, so some PSA increase seemed reasonable.
It seems that my model needs revision. I also have to decide by how much should I reduce the weekly dose, now at 25x4 mg/week, in order to keep my PSA around 0.05.
Update: 27 days later my PSA rose from 0.04 to 0.05 (different labs).
Since latest update I have halved the dose into two, or 2x25mg/week.
For this, I split a 50mg pill into two and take each half on Mondays and Fridays.
As I wrote elsewhere, during this period I tried to lower the Tamoxifen to 4x10mg/week.
Doing so, my breasts felt sensitive so I went back to a daily dose and this did the trick.
I am now within my initial target, i.e. 0.05-0.06 and will continue with 2x25mg/week.
From past observations I am aware that today's lab reports a tiny bit higher than that of the previous update. Consequently, I may have reached the sought equilibrium, but there will be a better insight after my next PSA test.
Since the previous update I have been taking 2x25 mg/week as before (one 50 mg pill split in two. The Bicalutamide blood concentration has long ago reached its steady state . Today's PSA was 0.05 like the previous one measured by the other lab. Today's lab had reported a 0.04 two months ago, but the Bicalutamide concentration at that time was 225% higher. My initial target to maintain a PSA of 0.05-0.06 according to some "Evolution dynamics" (thank you Nal) hypothesis, seems accomplished. Will keep taking current dose and monitoring results.
Six weeks after my latest draw my PSA remains stable at 0.05.
It seems that my feeble Bicalutamide dose of one 50 mg/week (25 mg on Mondays +25 mg on Fridays) has established an equilibrium. Yet, I am a bit undecided. The original plan was to have a PSMA PET/CT during summer when the pandemic deeps to its lowest. It is also desirable to have a PSA greater than 0.1 at the time of scanning for increased detectability. If I stop Bicalumatide now, it will take me one month to clean out and according to my prior PSADT ~9 months to double from 0.05 to 0.1, which brings me back the forecasted next peak of the pandemic. In my shoes, what would you choose?
a) Keep it as long as it works.
b) Stop it in September and get scanned sometime in spring-summer 2023.
c) Get scanned around my 3rd RP anniversary (late coming May) regardless of PSA value.
Hi Justfor,I don't think anything will show up on PSMA scan at those low PSA values. I was off of Casodex for 19 months and got a PSMA scan at PSA 1.27. The scan was negative. Anyway I started Casodex 9 days ago (50 mg/day). Today I had a PSA test that showed it dropped from 1.27 to 0.44 just in 9 days. I plan to keep PSA around 0.2 by adjusting the dose of Casodex. Ithink there is no need to lower PSA to almost zero (i.e. 0.03-0.05).
My bottle of Curcumin capsules, very conveniently, became empty in sync with my latest PSA test. I decided to abstain from opening a new one during this month in order to test whether it affects or not the PSA.. Having stabilized my PSA to 0.05 for 4 months now, a future increase to 0.06 will reasonably be attributed to the lack of Curcumin. Regardles, I will start again Curcumin next month. If it backs off to 0.05 again than this will constitute tangible evidence that Curcumin lowers PSA. Synergy with Bicalutamide or test masking, this is another story. Will report results.
Five weeks post my previous test, PSA remains stable @ 0.05.
As previously noted, this time I also wanted to check the influence of Curcumin on PSA.
For this reason I refrained from taking it all this time.
As of today I started taking it again.
The first leg of my "bracketed" experiment, i.e. ON-OFF-ON with Curcumin, suggests that the purported PSA lowering/masking effect is most probably a red herring.
My next PSA test will be definitive regarding this.
In my previous blood tests there was a substantial discrepancy in totalT between labA and labB. For a majority vote decision, this time, I used labC. Well, I got my answers regarding totalT but there was a discrepancy with PSA. LabC reports PSA to 3 decimal places, in this case 0.036 came back. The other two labs have been concordant with 0.05 for some months now. Just after the previous test I have restarted taking Curcumin, so there is a possible element there, although when I stopped it for more then a month PSA didn't rise. Plan now is to keep things as usual and in case next test (beginning of Oct.) using labA or labB prints the 0.04, then readjust the Bicalutamide dose.
I reviewed my supplements list for the period between the latest two PSA tests (0.05 -> 0.036) to notice that shortly after the 0.05 I added Glucosamine HCL (without Chondroitin). Among others, there are mentions that: "We and other investigators also have demonstrated the ability of GS to induce apoptosis in human cancer cells, such as prostate (DU145)...." spandidos-publications.com/...
It is the first time I am trying this supplement and it surely has attracted my attention now. First things first, I will have to verify that a genuine PSA reduction has occurred. In the past labC has been in very close agreement with labA.
This time the PSA test was carried out by one of the two labs that I usually interleave and they report to the second decimal digit. The result was 0.03 which after the previous 0.036 can indicate a declining trend. Since the first days of September last I have stopped taking Curcumin, yet continued taking Glucosamine HCL (without Chondroitin). Current PSA decline can be possibly attributed to the latter in an actual or placebo induced way. Alternatively, PCa cells got lazy and went for a nap. I will try to solve this dilemma by halving the Bicalutamide dose and doubling the Glucosamine HCL supplement. In order to get fast enough to the new steady state concentration (that of 25mg/week) I will skip one week of Bicalutamide altogether. Next PSA test in early November which is also the 1st year mark of these maneuvers.
Seems that my past dose halving to 25 mg/week was a bad idea that resulted in a rise outside my target range (0.05 +/-0.01). Initial, mid November, PSA reading was 0.074, retested with the other lab 0.09. I hypothesized two possible reasons for the rise:
a) There exists a min Bicalutamide concentration level, bellow which linear control is lost, sort of a hysteresis in control loops.
b) I had reached the point where Bicalutamide stops working, instead reverses and feeds PCa.
To find out what was happening I took for 10 consecutive days the nominal dose (50 mg/day or 350 mg/week) and today tested anew by the lab that reports to two decimal places.
It came back to 0.04 which is kind of very interesting, as when I started this experiment, a year ago, my PSA dropped from 0.17 to 0.09 after ten days of nominal dosage. Now 0.09 to 0.04 during the same time period and dosage indicate that my response to Bicalutamide is as good as it was a year ago when this was started.
Lastly, my calculations indicate that today's Bicalutamide concentration was equivalent to 30 mg/day of steady state supply, consequently, I am halving the dose until next testing.
Thank you for your kind response. It is the rounding to the second decimal place that doesn't allow exact comparisons between the two drop-rates. Both are approx 50%, give or take. I thought of using the lab that reports to three decimal places, for this reason, but the results of their last test were e-mailed to me the following day after the draw. If the analysis was delayed by one day, then with 3.5 days of half life for PSA, the two (0.074 and 0.09) come very close together. Hence, I opted for verifiable processing interval vs enhanced granularity. I think you would have done similarly.
Thirty five (35) days on half the nominal dose, i.e. 25 mg/day, and I got undetectable (<0.01). Three and a half years after RALP it is my first acquaintance to the less than "<" sign. Well, I must admit that I got lazy during the holidays. Last time I used this dosage, PSA declined from 0.09 to 0.06 within 10 days. I should have had taken the PSA test earlier, so I could re-adjust the dose accordingly and not derail my inner control loop. But, with daughter coming over from abroad for Christmas and the New Year, everything went astray. I understand that most, if not all of you, would brag for getting undetectable. Not I. As I wrote in another thread the stability of the power grid network is based on constantly balancing the power production to the instantaneous demand, also termed as generation to load. Too much production leads to grid collapsing like less does. Our body works the same. Produces Testosterone which, among others, is consumed by the cancerous cells. We have Bicalutamide that can sit in between the two and act as a control valve. Fully open or fully closed valve is anything but optimal. There is a mid setting that will maintain stability quite longer than either of the preceding. An engineer doesn't need any random trial to grasp this. It is just.... elementary.
Conclusion: I am re-adjusting the dose to 3x25 mg/per week and will re-test in a month. For newcomers to this thread my target is 0.05 +/- 0.01.
Forty (40) days at 3x25 mg/week (one and a half tab per week) and <0.01 still holds firm.
Late last week we had an interesting exchange with smurtaw and cujoe (healthunlocked.com/fight-pr... where, in accordance with a graph of my past performance, I guessed/estimated that this PSA count will be in the vicinity of 0.01. Backtesting proved correct. Borrowing a term from the nuclear science, my "critical dosage" is a bit bellow 50 mg/week. I am now considering halving the dosage on a bi-weekly schedule, i.e. Mondays and Fridays on week#1 and Wednesdays on week#2. This is equivalent of 37.5 mg/week. Hoping that this dosage will be more friendly to my hormone sensitive cells as hormonal cell cleansing is not a good idea.
Today, I was close the lab so walked in for a spontaneous PSA count. Long story short, stubbornly <0.01. Next step is dosage reduction to 25 mg/week and if this doesn't drive PSA above <0.01 then the BAT-like theory will become meaningful. Last time 25 mg/week tripled PSA in geometric increase, or shot-up 0.06 in linear terms (0.03 to 0.09).
This time I used the lab that reports to the 3rd decimal place. PSA at 0.015, came as a relief, as it dropped the undetectable "<" sign. The Bicalutamide concentration during this month has been ~80% of that of last November that derailed the control loop. Currently, I am undecided regarding the dosage to follow. I may maintain it as at present, that will probably increase next PSA count, or up it a bit that will probably stabilize or lower it. The thing I don't like with the latter is that there will be not enough visibility with the other two labs that report to the second decimal place. I will have to sleep on it.
I concluded last month's update with the line: "I will have to sleep on it". And indeed, it took me a couple of daytime-hours to decide upon the new dosage combined with a ton of algorithmic guesswork as to the projected PSA. When I say algorithmic guesswork, just imagine me pulling rabbits out of hats and squeezing them on the excel sheet with the historical data. Needless to say that the past three counts of <0.01 were not of any real help as they were not specific. Not to bother you any longer with my alchemy courses, I decided to increase the dosage by 50% (from 25 mg/week to 75 mg/2 weeks) anticipating a PSA of 0.018 to 0.022. Today's report came back at 0.020. Someone must be pulling my leg!!!
The good news is that my response to Bicalutamide is comparable to that of last year's. For this reason, this ongoing month I will be taking 50 mg (25 +25)/week like last year and monitor how it goes. The graph shows that both concentration and PSA went up this month, indicating a sub-critical dosage.
My algorithmic guesswork proved a total disaster. It predicted a slight rise, yet today's PSA test reported a slight decline from 0.020 (last) to 0.018 (now). More number crunching lies ahead. For this month dosage will be reduced to 44 mg/week, i.e. half a 50 mg tablet every 4 days. Google calendar app was set to remind me taking it.
This is all good stuff and I respect your diligence and approach (as a semi-retired consultant engineer working in pharma/medical devices). I think for most, their Consultant/Physician would not be impressed (they like to work by the book and you are stealing their thunder) but it's your body! Primary thought from my side is what is the state of your PC? You are using Bical to 'manage' your PSA, but as all on this journey (should) know - PSA level does not have a direct or linear correlation to PC status/progression. Have you had scans along the way that align with your 'control'? Also you occasionally mention the beloved parallel Tamox along the way - were you proportioning dose of that in parallel?
Firstly, thank you for your kind words. To answer your question now, I have had MRI and CT scans post RP but not PSMA PET/CT. This month's update will be of special interest as I have contracted COVID a few days after my latest one. All options are open: a) No interference of COVID with PSA. b) PSA rise as PCa progresses with inflammation. c) PSA decline if cancerous cells were collateral damages of the immune system attack to COVID and it's tails. Also, doc prescribed two courses of antibiotics to protect me from secondary pneumonia. Some regiments comprise an antibiotic to fight PCa. We will soon know.
A few days past the June PSA test I contracted COVID. I became curious to find out whether it would interfere with my PSA control system. I can report now that, so far, it does NOT. My July PSA came out as expected at 0.020. During this past month I have lowered the dosage from 50 mg/week to 43,75. Bicalutamide serum concentration declined to 84% that of previous test and as anticipated there was a PSA rise from 0.018 to 0.020.
For this past month I maintained the half tablet per 4 days dosage like the previous month. Then PSA had risen from 0.018 to 0.020 and projecting this I anticipated 0.021-0.022. But the analyzer, Abbot i Alinity ΜΤ-24-01 with advertised min PSA detection limit of 0.003, wanted to play games with me and the report came back at 0.005! I can see 3 possible explanations for that:
1) Machine with ageing calibration. It is early August and most people are preparing for their summer vacations. "A leave it as it is now and we will take care of it when we return in late August or early September" attitude wouldn't surprise me.
2) As has been observed in animal adaptive dosage tests, but also in my own case after equilibrium had been established during a couple of months last year, only to follow a PSA decline at same dosage, this is a pattern that can repeat itself again.
3) The long shot: Cardiologist prescribed a Beta Blocker to deal with Tachycardia induced by long COVID that I have faced with very recently. Before taking the new medicine I run it by Google to see how it affects PCa. The result of this search was a mixed bag, some claiming that it has some beneficial contribution others that it is totally unrelated.
Now the difficult part: Should I reduce the Bicalutamide dosage to half a tablet every 5 days, or continue with the existing one and put off any adjustment for September?
During August I decreased the Bicalutamide dosage down to 25mg every 5 days vs 25 mg every 4 days previously. On average, as there is latency involved due to the drug's long half life, the calculated Bicalutamide concentration dropped by 17% to 83% that of the August test. The PSA test came back at 0.011, thing that made me very happy. Going back to last month's post this rise in PSA points away from possible explanation 1) and more towards 2) or 3).
Hence, I did a search regarding Beta blockers and PCa and my findings are the following:
a) Early papers, up to 2015, find some benefit in Cancer Specific Survival (HR 0.78 and 0.85) without making any distinction between selective and non-selective Beta blockers. The one I am on is of the selective type.
b) Latest paper from Norway (2022) finds some benefit on BCR, but only for the non-selective variety.
c) There are another 2-3 papers that find no benefit whatsoever.
I will keep the current dosage during this month, as I would like to see how far up PSA can go due to inertia and seasonal change.
Closing last month's update I was anticipating a PSA rise that finally didn't materialize. Instead, there was a slight decline, all within the precision of the test. PSA went, a hair, down from 0.011 to 0.010 (same lab and such). Maintaining the same Bicalutamide dosage until the next monthly test during early November. For testing purposes I will double the Beta blocker dosage from 1.25 to 2.5 mg/day.
It is reasonable indeed. DHT follows, on a percentage basis*, the amount of total Testosterone in blood. I do take Avodart daily (Dutasteride) and on top of that drink a freshly juiced grapefruit that increases the bioavailability of it. The trick with the grapefruit amplification originates from a video by Dr Snuffy Meyers. (*) To give you some indicative numbers, my DHT was counted to 2.31ng/ml at the extremity of the total T of 3755 ng/dl making it 6.15%. The mean of 15 DHT & tT pairs is 4.77%, SD 1.57% ranging it within one standard deviation (SD) of the mean.
For a very-very short period (~2 weeks) I tried two tablets per day instead of one. Didn't notice any major change in DHT %, so dropped the idea. But, Avodart has a very long half-life taking months to establish concentration steady state. So, I am not sure if there is a dose related effect.
Seasonality and/or test variance out weighted any positive effect from the dosage doubling of the betablockers (everything else was kept unaltered). As of the 9th of November 2023 reported PSA is 0.016, a rise from the previous month's 0.010. Comparing that with last year's numbers, when there was a higher rise from 0.03 to 0.09 (different lab) but with the Bicalutamide dosage halved in between, the suspected seasonal variance seems becoming predominate. Current rise is welcome as my PSA target is 0.025-0.030. Thus, I will keep taking Bicalutamide at the current dosage (25 mg every 5 days) and if the PSA rise continues, so much the better. Driving into extinction all hormone sensitive cells is a BIG mistake. We need them to make life difficult to the resistant cells.
Last month's PSA rise turned into this month's decline. From 0.016 it dropped to 0.012. I take the same dosage since the 1st of August (4.5 months now) and PSA swings in the range of 0.010 to 0.016 (average of 4 tests 0.012). For this coming month everything stays as before. Christmas period, time to relax and get lazy.
Impressive journey indeed! Some questions, what does the drs say about this? And is there a risk that the cells get resistant to biaclutamide at some point?Are you still thinking of going through Psma pet scan?
1) I let the docs assume that I am taking the standard dose so a) they don't freak out and b) spare me their lecture. My life my decissions, not theirs.2) The theory of evolution claims that the more stress is applied to the hormone sensitive cells, the sooner the resistant clones will become dominant. That is what I am trying to avoid/postpone by limiting the dose to the minimum that maintains the equilibrium between those killed or put to sleep with the newborns. It is not the absolute value of the PSA that matters as most people believe and brag about undetectablity. It is the stability of the PSA that matters most IMO.
3) Of course, before salvage RT at a PSA over 0,2, after Bicalutamide has failed. When this will be, haven't the faintest idea. We will cross the bridge when we get there.
Was it your idea to go with the bicalutamide / dutasteride treatment plan? Are you dealing with a urologist or oncologist? Your efforts to actively manage your own treatment are laudable but like you say, likely to incur the wrath or disdain of your doctors. I am a retired engineer myself with a nodding acquaintance with control theory and such and I have a similar desire to tailor my own treatment and not just go along to get along. I've had a setback recently as I had to stop finesteride 5mg after it caused dental problems. I wonder if dutasteride would do the same.
Now that you mentioned it, when I started taking Avodart after RP, I noticed some discomfort at my lower jaw. I consulted a dentist at a cancer-only hospital as my family dentist wouldn't know the answer to my query which was: "Is it possible that PCa bone metastases can hijack the jaw?" Her answer was: " It can be, but haven't run across any. Do you take (named a drug) that is known to effect jaw necrosis?" No, I responded, only Avodart. She didn't show any interest to continue any discussion related to the latter.
Business as usual, i.e. PSA = 0.018, up from 0.012, 41 days ago. A very welcomed increase as relaxing the stress to the "good guys" (read the hormone sensitive cells) places roadblocks to the proliferation of the resistant clones. For this coming period, the 6th in a row, dosage will be kept at 25mg per 5 days.
As we are leaving winter behind, I was anticipating a reasonable reduction in PSA, but not that much. January's 0.018, had a free-fall to 0.009 40 days later. It must be the variability of the test along with the seasonal effect to account for such a steep change. I can't explain it otherwise. Nonetheless, I am taking a very conservative reduction on the Bicalutamide dosage from the current (since early August 2023 to be exact) half 50mg tablet every 5 days to half a tablet every 6 days. The five day period was easy to remember, seven, i.e. same day each week, is even easier, but I will go very conservatively here and elect the "difficult" six day period. The equilibrium is working oscilating around positive and negative PSADT values and any change should be very feeble not to derail it.
Lastly, in the back of my head I keep this passage originating from Dr. Bob Gatenby.
"An unexpected observation from the animal study is that, over time, this approach requires lower and lower doses to maintain control resulting eventually in stable tumors that required no therapy (the mice eventually die of old age)."
Who knows, maybe in the end I will append my nick name to Justformice.
This month, under latest dosage of half a tablet every 6 days, PSA has risen from 0.009 to 0.026. Not bad for a ballpark, but I will switch back to the previous dosage, that of half a tablet every 5 days. See you next month.
This past month I upped the dosage a tad to one and half tablet every 2 weeks, which is a hair shy of half a tablet every 5 days, i.e. half a tablet every 4.67 days. This schedule offers the ease of having 3 fixed days per fortnight in a 5+5+4 days succession. PSA went down to 0.022 from 0.026 previously. From the data I have collected thus far, it seems that the zero change dosage is about half a tablet every 5.5 days, which begs for an 11 day period in 5+6 days modulus. It's a bit an awkward schedule, so for the coming month I will continue with the current 5+5+4 and monitor for a PSA drop not lower than 0.018.
Anticipated slight PSA drop from 0.022 to 0.020 was observed, as current dosage is known to be over-critical. Will continue with the same, easy to implement, 5+5+4 schedule. The shallow decline trajectory (PSA velocity) of about -0.035/year, renders current dosage usable for a couple of months forward.
Layman here, however I recall reading that one caution in treating to a PSA level is that some forms of PCa don't raise PSA as much as others. Thus PSA testing is very useful, however it is not a 1:1 measurement of PCa. This is the reason for the manual digital screening exam with the PSA test: IIRC 85% of PCa is detectable via PSA tests -- which leaves 15% unaccounted for. I gather some PCa cell types don't leak PSA as much.
Yes, there is certainly such a risk. But what is the alternative? Let PSA rise to say 0.1 or 0.2 and have a PSMA PET scan? Risky as well because when the genie gets out of the bottle, it is difficult to get it back in. Finally, as I have thought of it since some years now, I have decided to take that risk. Thanks for your consideration.
Last year (2023), commenting on my PSA test (10 days later than now - early August), I wrote:
"Scratching head time. For this past month I maintained the half tablet per 4 days dosage like the previous month. Then PSA had risen from 0.018 to 0.020 and projecting this I anticipated 0.021-0.022. But the analyzer, Abbot i Alinity ΜΤ-24-01 with advertised min PSA detection limit of 0.003, wanted to play games with me and the report came back at 0.005! ".
It seems that history repeats itself as a farce, because today, while projecting a 0.012 to 0.013 PSA got 0.006!
I have another thread, where I document a PSA winter/summer seasonality, but this 0.006 goes far beyond this. Is it the ambient temperature, sea bathing, what???
Dosage has been fixed since early April 2024 complying to the 5 + 5 + 4 day schedule. I didn't do any dose adjustments exactly for this reason.
Your work is interesting to me since I have been throttling my Bical for several years.
But with your RP and lack of metastases(?) how do you know whether the very small PSA changes you get are due to the different Bical timing/dosages or just random variations in testing coupled with the fact that you do not have any (or few) producers of PSA left in your body?
I just don't know. But I take care not to drive into extinction all hormone sensitive cells. That's why I want to keep a residual PSA and undetectable is a no-no for me. Keep them from uncontrollable growth, NOT force them to evolve into hormone independent ones. You are a law abiding citizen and pay your income taxes, right? What would you do if your government one day passed legislation raising the income tax coefficient from say 30% to 100%. Do you think that you are smarter than your cells?
Continued excellent work and shares! I too can scratch my head, holding 0.03X over three years now, no drug interventions, and five years since completion of one year on bical, full dosage 150mg daily.
I have a simple thought - 'somehow', gratefully, we may be approaching a measurable degree of durable remission, because our remaining cancer (currently) has insufficient volume to support growth and to spread. I do ponder - is this sustainable without further interventions?
Reasonable thoughts. You have achieved equilibrium without external hormonal intervention. Along this scenario I am a step behind you. I need to resort to some Bicalutamide for keeping the bad guys at bay.
Getting back on bical is always in my quiver - and I do ponder should I be on it now? Why I PSA test monthly to bi-monthly and have added annual liquid blood biopsies and imaging.
I was right to be suspicious regarding July's very low PSA (0.006). Two months later (in between I was by the sea, so no labs during August) PSA came back at 0.007 which, knowing that the current dosage is over-critical, aligns better with my estimates. Consequently, I can now lower by a tiny-tiny bit the dose, to half a tablet every 5 days, hoping that this will drive the monomers to pair, formimg dimers (according to the recent paper) and eventually rise my PSA above 0.010.
Hi just for thank you so much for the detailed testing. After using ivm for a year psa is increasing from a low of .65 to 1.5 and psma scan shows medial lymph node and hip bone met, very small and RO gave me the option to wait n see but I pushed for Sbrt to the locations. I’ve always thought if Ivm is not powerful enough then I will try the bical per your posts over the years. So I’m curious to what your thoughts on which route I might want to go from here. Mo did rx bical for me and wants me to take it whether I do the radiation or not, again what’s your thoughts Tia …
3) Bicalutamide 25 mg (half a tablet) every 5 days,
4) Tamoxifen 30 mg per 5 days as 10 mg on the Bicalutamide day and 5 mg the remaining four. The Tamoxifen titration is very recent as in the past 3 similar attempts had been aborted when within a week I felt tenderness in my breasts.
Supplements:
Vitamins D3 and K2, Berberine, Fishoil Omega3, Theracurmin, Milk thistle, Quercetin, Melatonin, freshly juiced Pomegranate when in season.
Thank you very much for your reply. Do you use the statin to block cholesterol as a precursor of the steroid hormones or just to reduce the cardio-vascular risk?
Do you use high dose Melatonin or 1-3 mg as usually recommended?
I have, geneticaly confirmed, familial hypercholisterolaemia. Total Cholesterol without statins north of 320 mg/dl. Converted in bulk to Testosterone. My baseline T, before any medication, was 800-900 which is 99+ percentile for age.
Melatonin in mega dose: 2x10mg before going to bed (smiling face here).
I heard people with cancer take up to 60 mg of Melatonin, so 20 mg is not the upper limit.
I assume you take Berberine as a natural alternative to Metformin? It has a potent anti-microbial effect, so it may be worth adding probiotics every now and then to keep microbial diversity in the gut. Also eating vegetables and protein first before carbs will reduce glucose (and insulin) spike .
Thank you for your advice. Please keep updating us on your progress!
Yes, you are right, However, Justfor’s approach is logical, thorough and personalised. He addressed the issue from every angle including precursors and metabolites. I am going to use his regime to hopefully minimise the side effects of the AR inhibitor
"Bicalutamide Clinical Pharmacokinetics and Metabolism" by Ian D. Cockshott, AstraZeneca, Macclesfield, UK (Clinical pharmacokinetics, 2004-Springer)
It is evident that among 116 men under the standard dosage of 50 mg/day the spread of serum Bicalutamide steady state concentration was ~16X (1.38 - 21.7 mg/L). Consequently, under the silly dogma of "one dosage optimal for all", some will be under-treated, while others over-treated.
This is why I don’t view your success as a miracle, but as an intelligent scientific calculation. This gives one hope that it is replicable (subject to correct calculation of the dose).
Have you ever thought of personalising the Dutasteride dose by measuring DHT, considering its half life is 5 weeks?
Yes, I once tried and doubled for a month the daily Dutasteride dose, but my DHT counts have shown quite a tight ratio with total Testosterone averaging to 4.8% (3.2% - 7.2%) whatever tried. Didn't find any useful correlation, apart from the fact that Dutasteride rises Testosterone and as a consequence DHT in absolute terms. Instead, after watching a video by Snuffy Meyers saying that a glass of grapefruit juice increases the bio-availability of Dutasteride, I am combining grapefruit juice with Avodart during breakfast, but unfortunately the ratio of DHT/tT remains stubbornly unchanged. But, I like grapefruit juice and whether it works or not is irrelevant.
Don’t have the juice on empty stomach as it’s full of fructose, which quickly converts to easily available glucose, followed by an insulin spike. And we all know that hyperinsulinemia stimulates 5 alpha reductase activity and T-to -DHT conversion. In other words, grapefruit juice inhibits P450 making Dutasteride more bioavailabe, but stimulates 5 alpha reductase through the back door by increasing insulin
Thanks for the heads up but I think I have me covered by taking Dutasteride with breakfast, Berberine and grapefruit juice.
ChatGPT comments as follows regarding this combo:
"Taking berberine with grapefruit juice presents a potentially interesting combination, but there are a few important considerations to keep in mind regarding both metabolism and potential interactions.
1. Berberine’s Effects on Metabolism
Berberine is a natural compound that has been shown to help regulate blood sugar levels, improve insulin sensitivity, and may reduce hyperinsulinemia. It works by activating AMP-activated protein kinase (AMPK), a key enzyme involved in energy metabolism. Berberine has effects similar to the diabetes drug metformin in terms of improving insulin sensitivity and glucose metabolism.
Berberine and 5-Alpha Reductase: Although berberine can improve insulin sensitivity, there is no direct evidence to suggest that it affects 5-alpha reductase activity or testosterone-to-DHT conversion. However, by improving insulin sensitivity and reducing hyperinsulinemia, it could indirectly reduce 5-alpha reductase activity, since high insulin levels are associated with increased enzyme activity.
2. Grapefruit Juice and CYP3A4 Inhibition
Grapefruit Juice’s Inhibition of CYP3A4: As previously mentioned, grapefruit juice inhibits the CYP3A4 enzyme in the liver and intestines, which can increase the bioavailability of certain medications or compounds metabolized by this enzyme. Berberine is partially metabolized by CYP3A4, so drinking grapefruit juice alongside berberine could potentially increase the concentration of berberine in the bloodstream, enhancing its effects.
3. Potential Benefits and Concerns
Potential Benefit: The combination of grapefruit juice and berberine could theoretically lead to increased bioavailability of berberine, making it more effective at lower doses. This is similar to how grapefruit juice affects the bioavailability of other compounds like dutasteride or certain statins.
Risk of Overdosing: While berberine is generally considered safe at recommended doses, increasing its bioavailability through grapefruit juice could enhance its effects to an unexpected level. This could lead to gastrointestinal issues (common with higher doses of berberine) or even interfere with its regulation of blood sugar levels, causing hypoglycemia in sensitive individuals.
4. Combining the Two: Is it Safe?
Caution Advised: Because berberine is metabolized by CYP3A4, taking it with grapefruit juice could alter its absorption and effects. While this might seem beneficial, as berberine would become more potent, there is also a risk of unpredictable interactions and side effects. Additionally, if you're taking other medications that are metabolized by CYP3A4 (such as dutasteride, statins, or blood pressure medications), the combination could lead to drug interactions.
Conclusion:
If you're considering taking berberine with grapefruit juice, keep in mind that:
The combination could increase berberine's bioavailability, making it more potent.
Grapefruit juice may affect the metabolism of other drugs you are taking, leading to possible interactions.
A healthcare professional should ideally be consulted before combining these two, especially if you're on medications or have pre-existing conditions like diabetes, as the effects on blood sugar could become more pronounced.
It's important to monitor the dose and effects carefully if you go ahead with this combination."
First off, check your sensitivity to the drug. PSA test, followed by 10 days at nominal dosage 50 mg/day and retest. I am a good responder and twice my PSA declined by about 50% doing that. Others, that I know of, were not that sensitive. Sensitivity from person to person can vary 10fold. Let me know your PSA decline and I will guestimate whether you need to keep up with the nominal dosage or you can adjust it lower and by how much. I have devised an algorithm that (supposedly) can provide some guidance, but don't swear on it. Doing that don't change anything that you are already doing. Only add the Bicalutamide to your current regimen.
My PSA is mimicking the punctual behavour of a Swiss train. 40 days ago I reduced my dose by 7% (from 5.36 to 5.0 mg/day) and thus PSA has risen by 14% (from 0.007 to 0.008). I am still a bit south from my min target >0.010, but considering the seasonal nature of my PSA I anticipate to achieve it by November (3rd anniversary) or tops by December maintaining current dosage. If you are a new reader here, you may be taken aback by the verb "achive" I used in the context of a PSA rise. It is NOT a typo and my English isn't that bad. I want my PSA to be within the bracket of 0.010 to 0.050 so that, like today, I can gauge that Bicalutamide is doing its job. Undetectable "achievements" are only good for silly docs and their unfortunate patients. Just think how you test that the engine of your car functions properly. Don't you step-release the gas pedal and monitor the sound of the engine as it ramps up its RPMs?
Great piece of information Justfor_. I presume there are many of us watching your ongoing progress. Thank you for your continued updating of your personal trial.
One and a half month before I was writing: "I am still a bit south from my min target >0.010, but considering the seasonal nature of my PSA I anticipate to achieve it by November (3rd anniversary) or tops by December maintaining current dosage."
The Swiss train in me delivered and I am most happy to share that today's PSA count was 0.010. Can't convey you my enthusiasm seeing that my feedback loop functions as anticipated. Consequently, dosage stays as before for the next 1.5 month to come.
Last year, under the same dosage, my PSA spiked up like this:
13_Dec_24 -> 0.012
23_Jan_24 -> 0.018
4_Mar_24 -> 0.009
This year:
11_Dec_24 -> 0.010
27_Jan_25 -> 0.021
But, the most intriguing thing is that for the last two years there has been an inexplicable deep during late June - early July. There are posts above with details, if anyone is interested.
Dosage stays the same to check if the pattern repeats into March.
I had noticed my PSA seasonality before starting with adaptive Bicalutamide. During that period, it wasn't the constantly rising PSA but the PSADT that presented seasonal characteristics shrinking during winter and easing during summer.
For this month I was expecting a lower PSA, but instead, I got 0.030 from 0.021 45 days ago. Currently, a nasty stubborn flu is upping inflammation and this may be a contributing factor to the "elevated" PSA. Will maintain same dosage ("frozen" since September 2024") and see what April will brink up.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")