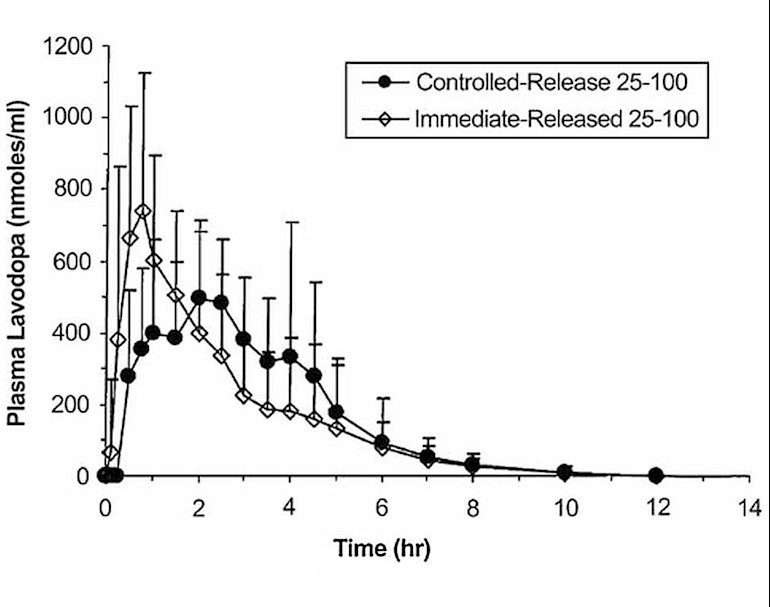
The question of immediate release versus controlled-release carbidopa levodopa is a frequent topic here, so it is high time to have a post specifically addressing this issue. Chart source: ingentaconnect.com/contento...
With reference to the above chart, if a person is dosing at 5 hour or greater intervals, the controlled-release formation provides a much more even level of levodopa. On the other hand, if a person with more advanced Parkinson's is dosing at 4 hour intervals or less, the immediate release version is more appropriate, because the controlled-release levels will overlap, causing a "stacking" effect of increasing levodopa levels.
To get a graph of your Levodopa Equivalent Plasma Levels, use the excellent application created by fellow member johntPM, available at this link: parkinsonsmeasurement.org/t...
Regarding food, according to the Sinemet CR label: dailymed.nlm.nih.gov/dailym... "The extent of availability and peak concentrations of levodopa after a single dose of SINEMET CR 50-200 increased by about 50% and 25%, respectively, when administered with food."
Also from the label: "In elderly subjects, the average trough levels of levodopa at steady state after the CR tablet were about 2 fold higher than after the standard SINEMET (163 vs. 74 ng/mL).... In these studies, using similar total daily doses of levodopa, plasma levodopa concentrations with SINEMET CR fluctuated in a narrower range than with SINEMET. "
Update 10/21/2021 - CR vs IR, the Debate
I personally favor the controlled-release version. By all means those who are better served by immediate release should continue with it.
It is not true that immediate release is always better. Doctors tend to prescribe immediate release by default, for infrequent dosing, without educating the patient as the pros and cons of the different versions, and this is wrong.
This study followed 618 patients over a period of five years. Half of them took CR and the other half took IR Sinemet:
pubmed.ncbi.nlm.nih.gov/901...
It found:" Activities of daily living scores in the Unified Parkinson Disease Rating Scale (UPDRS) consistently favored the Sinemet CR treatment group and a number of the NHP scales also favored the CR group. ... There was a statistically significant difference (p < 0.05) in activities of daily living as measured by the UPDRS in favor of Sinemet CR." On other measures the results of the two formulations were similar.
Since publication this study has been cited 304 times by various researchers:
scholar.google.com/scholar?...
I did not see any of these contradict the above study. So is has stood the test of time.
If doctor's opinions were as good as double-blind studies we would not need to bother with them. That is not the case - investigator bias is all too real a factor, and an M.D. busy in clinical practice is not in the position to carefully test, monitor and tabulate results, particularly of similar reasonably good treatments. Opinions are not evidence and that includes the renowned Doctor Ahlskog. He alleges the following drawbacks to the CR formulation:
"1. Effect: 60-90 minutes longer than regular carbidopa / levodopa
2. Slow to kick-in and more erratic
3. Complex interactions with food
4. Not a mg-to-mg correspondence with regular carbidopa/levodopa"
Taking these point by point:
1. Yes that is the point of CR which is why it is better for infrequent dosing
2. Yes it is slower to kick in. We take levodopa on a schedule, which allows for time needed to kick in. We do not wait for the moment we think we need another dose. I have not seen any evidence that is "more erratic"
3. No evidence cited to support this allegation
4. True it is not a milligram to milligram correspondence. It is is a simple matter to take a bit more. Better yet, simply starting with the CR version moots the issue of needing to find an equivalent dosage.
Further details for data wonks:
In searching for the appropriate chart, there were an excess of hits for "ER CD-LD", which is actually Rytary and therefore not relevant to the discussion. The terminology used in the title for this post follows that used in the reference for the chart. The actual names for medications are "Sinemet CR" for the original medication, and "carbidopa levodopa ER" for the generic.
More from the Sinemet CR label: "In healthy elderly subjects (56-67 years old) the mean time-to-peak concentration of levodopa after a single dose of Sinemet CR 50-200 was about 2 hours as compared to 0.5 hours after standard SINEMET. The maximum concentration of levodopa after a single dose of Sinemet CR was about 35% of the standard SINEMET (1151 vs. 3256 ng/mL)."
These levels are different than the chart because dosage used here was twice the dosage in the chart. Note in the chart that peak CR level is 67% of that of the IR formulation vs. 35% per the label. This discrepancy is due to different sources of data – the chart comes from "database within IMPAX Laboratories, Inc., based on studies conducted by IMPAX Laboratories", whereas this Sinemet label comes from the Sinemet sponsor Merck Sharp & Dohme Corp. Adjusting for different dosages, the CR levels are comparable, but the peak IR level measured by Merck is about twice that measured by Impax. I am inclined to credit the Impax number because I have not seen information elsewhere that supports the Merck number.
Continuing with the label text: "The extent of availability of levodopa from Sinemet CR was about 70-75% relative to intravenous levodopa or standard SINEMET in the elderly. ... Because the bioavailability of levodopa from SINEMET CR relative to SINEMET is approximately 70-75%, the daily dosage of levodopa necessary to produce a given clinical response with the sustained-release formulation will usually be higher."
Update 6/2/2023 - Gender Differences in Plasma Levels
see: healthunlocked.com/cure-par...
Update 1/29/2024
The foregoing concerns plasma levels of levodopa. That is not the same as the level of dopamine in the affected neurons. There is a delay getting through the blood-brain barrier, and another delay turning levodopa into dopamine. Following that, the dopamine persists for some time. I've noticed I still receive some benefit even hours after my plasma levodopa is gone.

") However, I see that you appreciate the research done by Italians on dyskinesia , excellent preference. Like the artist of your avatar, very refined, Gustav Klimt the only recent artist I appreciate.
However, I see that you appreciate the research done by Italians on dyskinesia , excellent preference. Like the artist of your avatar, very refined, Gustav Klimt the only recent artist I appreciate.