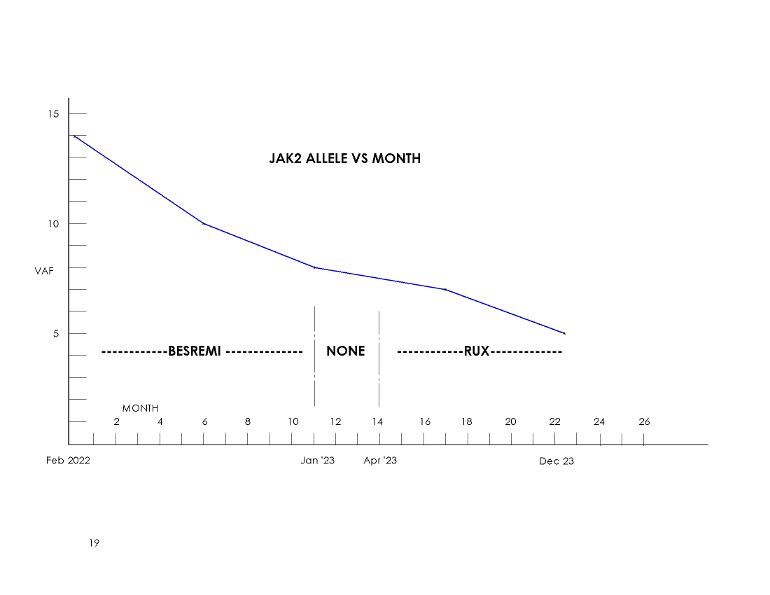
I got my latest Jak2 update. The plot shows what is going on, a nice continuing reduction to 5%. My allele on IFN appears to be leveling off, suggesting a best value over time of maybe 6% if that had continued. The surprise is the steeper drop resumed on Rux. This continues to match my Dr's opinion that Rux is good stuff.
There are two members now reporting Rux VAF reductions consistent with the recent trial reports: Member Sewingtime has 60-25% over two years on a low dose.
I've held CHR on all three MPN meds; for VAF reductions on IFN having CHR is a correlation. I believe it's similar for Rux if I recall right.
Of course we can't know what my IFN would have led over more time. Same for future Rux readings. We have seen that IFN can reverse slightly to increase VAF at some point, usually on average after ~5 years, I'd guess Rux could do the same but it's not been studied this way yet.
As always, at what level if any does it matter? Could one go off Rux at very low VAF levels?
My test result has this note I've not seen before "The sensitivity of the assay has a lower limit of detection of 1% mutant alleles in a background of normal alleles, and it is not designed to distinguish heterozygous from homozygous mutations."
So if I have good fortune to approach 1% (unlikely) this test will start to lose accuracy. As in prior posts homozy associates with higher VAFs (50%+ for example) and responds better to IFN. This is probably why we see steep initial reductions here on IFN from the higher values. At 14% at Dx I more likely had heterozy.
Anyway I'd gladly trade some allele for Sjogren's relief any day.(not that there is any connection)

 he's only on blood thinners and beta blockers at the moment, should he be on something to reduce his alle frequency? I don't really understand it that much but i believe the lower it is the better?
he's only on blood thinners and beta blockers at the moment, should he be on something to reduce his alle frequency? I don't really understand it that much but i believe the lower it is the better?