Just want to share my Besremi experience for anything to be learned from it.
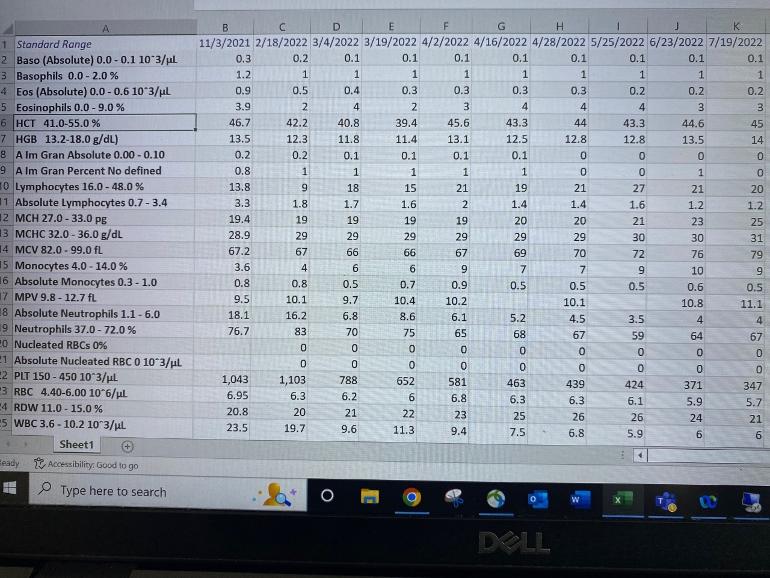
Above picture shows my CBC after the 11th dose (results of 7/19/2022; 1st dose results was on 2/18/2022).
HISTORY: Diagnosed with PV 4 years ago; JAK2 positive with very low erythropoeitin; I am now 64 years old; Only phlebotomy and aspirin for 4 years until Besremi in Feb 2022. Most concerning before Besremi was platelets of 1100. Allele Burden was 70% before Besremi. Currently, other than low-dose aspirin, Centrum 50+ men's vitamins, and garlic suppement plus raw 2 cloves of crushed garlic every other day; I have no other medication. I have been wearing CPAP mask for sleep apnea since year 2000.
BESREMI EXPERIENCE: Very good to excellent results - so far. After the the 11th dose of 175 mcg (1st at 100, 2nd and 3rd at150, and 4th, 5th, 6th , 7th, and 8th at 200, 9th and 10th at 175 mcg), Platelets down to 347, WBC and HGB in normal range coming from a high number. HCT was 45.0. Pruritus had been absent since the 2nd dose of Besremi, but it is coming back with minor inconveniene only.
BESREMI SIDE EFFECTS: After the 11th dose, first 48 hours after injection, a flu-like symptoms but manageable and no medication required - lately it has been almost negligible.
OTHER CONCERNS: Low MCH, MCHC and MCV. My research points to low iron stores as the reason for these non-normal values. The CMP results/report all numbers in normal range except carbon dioxide at 32 (one over the normal range). Iron/Ferritin test show moderately low values for a few (iron) parameters; but trending toward better numbers.
If interested in historical comparison of CBC counts, please see related previous postings.
God Bless and All the best to everyone!
Written by
Pat032018
To view profiles and participate in discussions please or .
Quite nice CMPs. Your liver numbers are normalized, I recall you said these were high. Your provider has much stricter AST, ALT upper limit than mine, (62, 70) I'm at 38 AST which is near yours but mid range in my provider plots. It suggests there is a lot of wiggle room here, and we know Bes allows up to 3X these values at least for a time.
I hope that my AST and ALT do not go out of range again. I am watching my wine and beer consumption; and also my use of alcohol-based hand sanitizers against covid as I am one of those who developed OCD (compulsion) to have my hands 'sanitized' during this pandemic. I washed my hands or sanitized it in an unbelievable frequency.
Your lab must be using another measuring system for ALT and AST but I imagine these numbers will equate properly (if measuring units are different).
I think they are same units U/L, here is my related results. If so it brings up interesting point, that we seem to be meeting different standards on these two. But you're right my provider is an outlier.
Looking online at various providers, I find a max value of ALT=36 to 56, AST=33 to 48 and this qualifier is common " Normal results vary from laboratory to laboratory" They sure do.
My provider in contrast uses a tighter range for PLT (370max), but the difference is more striking on the two liver number ranges.
Thanks for sharing that. My hematologist just said that "we will monitor" when I had an elevated ALT and AST, but then I went back to normal range on subsequent testing one-month later.
That is certainly a very favorable response to Besremi.
I expect you are correct about the iron deficiency issue. Your iron levels should slowly improve now that you are no longer doing phlebotomies. Unfortunately the phlebotomy-induced iron deficiency can have significant adverse effects. It caused me fatigue, decreased concentration, and reactive thombocytosis (+200). I feel much better now on Besremi with higher iron levels.
All I did was to avoid HU for as I long as I can; and the FDA approval of Besremi in November 2021 coincided when I badly needed cytoreduction at over 1000 PLT count/level late last year. I once mentioned to my hematologist (who was very receptive - and he is in your list of poviders specializing in MPN) that I wanted to defer using HU for a as long as I can.
I would have taken HU if not for the availability of Besremi - in my case availaibility was around February 2022 including the approval process.
My current HCT is at the margin at 45 and I might increase Besremi from 175 to 200 mcg on my next injection. I hope my HCT remains at a level where I would not need phlebotomy.
My iron is improving. I once declined my hematologist suggestion to take iron pills and responded by intentionally finding foods rich in iron.
Nothing is guarenteed in our PV journey. I am thankful that things are getting better for me. God Bless us all in our journey!
I cannot thank you enough because I followed your articles as you provided excellent insights into MPN and have shared important and relevant articles. My former and first hematologist in California (and I moved out of that state), did not have the time for good discussions with me; and that I learned a lot more from reading here. After moving to a university connected hematologist, I realized that my Cal based practitioner, in solo practice/not connected to a health-care network, was always busy and did not have time even though he is knowledgeable. Lesson learned here was that I will no longer select a 'private'/solo practitioner because all I got was (at most) 10 minutes from the him/her during my office consultations.
I do know the perils of what I call "15-minute Doctors." Each patient gets 15 minutes, including the time to document the session. Line then up and march them out. It works OK for minor issues but not for more complex situations when there are always questions. Glad to hear you landed in a place where you can get your questions answered.
Glad you were able to get Besremi approved. I agree that it is a much better treatment option for PV and likely other MPNs too. It is unfortunate that it is so expensive that many people will be unable to access it. Getting it approved can be an uphill battle too. I had to put a lot of work into getting the authorization.
My HCT popped up above 45% - to 46.3%. The MPN Specialist and I upped my dose to 150mcg and then were patient. Took several doses but it came back down to target. The doc was more concerned about the Neutrophils not dropping too low than by being a point above 45%.
It looks like the Besremi is doing a great job controlling the Erythrocytosis, Thrombocytosis, and Leukocytosis. Thoughts and prayers headed you way for continued success on this journey.
The "documenting" you mention has been a big hassle for Drs since e-records started. My MPN Dr recently got a scribe helper so he doesn't touch a keyboard during visits. Seems helpful, but still just the ~20 min visit. My cardiologist was jealous; he'd heard about it but can't get one.
Several of my docs now use a medical scribe, either in the appointment or a virtual service. It is great as it gives the doc more time and ability to focus on the patient.
Your numbers are looking great! I can’t wait to get started. Ready to see positive numbers for me too! Sounds like you are doing great! Thanks for sharing!
Thank you Soledad (BTW, I like this name). Yes. I noticed that, but I do not know. I had a sprain knee from sports activities and have not been exercising as I used to; reading about it, the lack of my usual physical activity could be a causeof higher carbon dioxide. That was the first time ever when that CMP item went out of range; and I hope it is just one-off.
Hi Soledad. I do not know. Carbon Dioxide test is a standard item within the Comprehensive Metabolic Panel Test. In my case, I noticed it because it was outside the normal range; and then I went to Google it for what it means. I am not in the medical field and I have to research on these testings.
Hi Pat- it's unlikely that your serum CO2 has anything to do with your activity levels, it's more likely a response to your overall systemic pH balance.
If it were a significantly elevated value and you had chronic lung disease [COPD like Emphysema or Chronic Bronchitis], they could be the underlying cause.
But the blip [fancy medical terminology meaning a very slight and likely temporary deviation from under the bell curve] that your labs showed is very unlikely to be indicative of anything at all- unless it becomes persistent and progressive.
We all need to remember that the normal ranges are average that were taken from large populations of various individuals, so sometimes we [as other individuals] can be at one or the other ends of the so-called normal bell curve, and that each result is single snapshot of a much more complicated process.
For those reasons, I almost always prefer to look at lab results in graphic form, which is much better at demonstrating trends [or ruling them out].
Your take sounds much more credible than what I read from my Google searches. I will wait for next month which will provide me a 2 month trend - even though two months is probably an insufficient length of time to form a trend. Thank you.
He will not normally recommend it. I will have to request it and that will remind him. The insurance company will be contacted for coverage before scheduling the test.
My favorite plot shows what might happen. This is from the Ropeg (Besremi) study. Studies of PEG showed similar decrease pattern. On average any progress will be clear during the 1st two years. But these are median results and individuals vary of course.
I think I may get checked after one year (Feb 2023)
Here is the article. But it seems for these reports there is always something missing.
This part has been updated to 20.7% in other reports at 6 years, so a good trend continues:
<<allele burden decreased to <1% in 18/92 patients (19.6%) receiving ropeginterferon alfa-2b>>
One missing item is the allele plot at 6 years, it goes to 60 months only. I've been seeing evidence that INF can lose some allele benefit starting at 6 years, and esp at 7, I've posted on it before. Could be Besremi has improved on this, see "good trend continues" above.
I totally agree on plots. My provider has my bloods available this way on the portal, very convenient.
The Ropeg plot you see above was not actually available till recently, quite strange. I made one myself last year from the trial data, it's on some earlier posts; either way it's the right way to see things.
Plots are good for taking some of the fright out of outlier results.
FYI, you previously asked about my BMB results, but I had to remember to pull them up so I could share them- also, even though it was performed on 7/11/22, the results are still trickling in.
For example, I just found out yesterday that my JAK2 allele burden is 39%.
Here are some of the other highlights:
FINAL DIAGNOSIS:
**CYTOGENETICS ADDENDUM DIAGNOSIS 07/26/2022**
KARYO DIAG 7/11/2022
SUMMARY:
No Evidence of Clonal Aberrations
**ADDENDUM 07-14-2022**
Reticulin stain is negative for increased reticulin fiber deposition
Red blood cells: Normocytic normochromic anemia with mild anisocytosis
[the medical term for having RBCs that vary in size beyond a normal limit]
and
polychromasia-
[Polychromasia occurs on a lab test when some red blood cells appear bluish-gray when stained with special dye. This happens when red blood cells are immature because they were released too early from your bone marrow. These immature cells are called reticulocytes]
Lymphocytes: Small & mature
Neutrophils: Unremarkable
Platelets: Unremarkable
ASPIRATE SMEARS
Quality: adequate
Cellularity: increased
Myeloid:erythroid (M:E) ratio: normal, 2:1
ASPIRATE DIFFERENTIAL COUNT 200 CELLS COUNTED
Blasts: 1
Promyelocytes: 3
[granulocyte [WBC] precursors, developing from myeloblasts, then developing into myelocytes]
Myelocytes: 5
Metamyelocytes: 6
[Myelocytes, along with metamyelocytes and promyelocytes, are the precursors of neutrophils, the largest class of WBC]
Bands: 19
[Immature WBC]
Neutrophils: 17
Monocytes: 5
Lymphocytes: 14
Eosinophils: 1
Basophils: 0
[the 5 cell types above are the various WBC types]
Plasma cells: 1
[type of immune cell which makes large amounts of a specific antibody. Plasma cells develop from B cells that have been activated. A plasma cell is a type of white blood cell.
Erythroid: 28
[pertaining to RBCs]
CORE BIOPSY
Quality: Adequate
Length evaluable marrow cavity (mm): 12
Cellularity (%): 80% with panmyelosis
[Tri-linear hyperplasia [overproduction] by bone marrow]
Myeloid:erythroid (M:E) ratio: Normal
[WBC to RBC cell line]
All in all, nothing unexpected, but [obviously] I'm happy that there has not been any apparent progress to Myelofibrosis.
..that's my story and I'm sticking to it.
😎
To Pat,
I'm sorry for the thread highjack, but I just couldn't find the post where EPguy asked about my BMB results, and this was his most recent reply to me.
I found the prior thread, but with Pat's approval, comments here:
That report is a super high level of detail that I think is rare. MF 0 is great. Blasts at 1 would be 0.5% I don't know what that means, but I've seen blast % noted in reports. Mine had "No increased blasts", but no mention of increased from what base level. Any comments on the 200 cells result, and other data, from your Dr would be interesting.
AB of 39% is right in the PV range. No mention of other mutations, a good thing.
I've not heard of polychromasia before.
Tri-linear hyperplasia I believe is a classic PV criteria. This is where my Dx gets mixed, I had ET style features here, only one of the three- "Megakaryocytes are increased...".
Cellularity at 80% is over the 70% that I found is top range normal for adults, and is typical for PV. I also had hypercellularity but no % provided. I have this question ready for my Dr.
As it happens, I had a f/up visit yesterday w/ these pertinent CBC -results:RBC 5.9 [nml]
WBC 10.5 [^ mildly]
Platelets 195K [[nml]
Hct 47%*
*So of course I required phlebotomy, where unfortunately [and unusually for that office], the RN seemed pretty unexperienced and inept, and achieved only a tenuous vessel entry.
This was in spite of my having showed her where most of the RN's manage to get vigorous return, which in retrospect, I think was because she had angled IV catheter just wrong, perhaps in addition to driving it too deep [it was hubbed and while I'm a big guy, my veins aren't deeply buried at all].
The end result of this was that, in spite of the other RN's guiding and assisting her, the IV kept getting clotted off, despite them flushing and moving it about multiple times, we managed to drain about 440 ml vs the ordered 500 ml- not too big a deal, but that was over approx. 2.5 hours of her endeavors.
My MD was cool with having an MPN expert consultation, and will be sending a referral letter summarizing my history and care thus far, and although her reported plan was to change to Jakafi, if my response to HU continued to be sub-optimal at 500 mg/day.
She said that she was concerned that my platelets would tank if we increased the HU dosage, and in addition, she was sensitive to my concerns about skin Ca, and other HU- associated cancer development.
My doc said that my karyotype, [which only looks for other general genetics whoopsies was nml- 46 chromosome yaddda yadda], but that the more specific screening for so-called 'non-driver' mutations is still in processing.
Next f/up will be in 2 weeks- but despite Pat's kind forgiveness of my thread-jacking [Thanks again!!] I'll start a new thread at that time.
Hi PA, Are you in USA? Is there any reason why you and your Hematologist are not considering Besremi yet? By recent experience of few to many folks including myself in this website, I hear mostly (if not all) positive results for Besremi. Hope goes well for all of us!
Wow, that's an awfully personal question! [Just kidding ]
Yes, and I have been pushing hard for changing to Besremi, but my General Heme/Onc MD admitted that her specific experience with PV was at best, very limited, and as a result, her experience using interferons [especially the newer formulations] to treat it is non-existent, but also that the experience she has had with it in general oncology was that patients had real difficulty tolerating it.
That's why I have been sending her the articles I find that draw a sharp contrast between outcomes on Hu and interferon, as well as those about the significantly improved tolerability both of the newer formulations, and of the lower doses needed for control of PV.
In fact, I brought up the subject at our 1st appointment, and have not recanted in the slightest since, mainly because I want to live as long as possible and in as healthy a condition as possible.
...and to her credit, she readily admitted her limitations, and more importantly, stated explicitly that she would happily participate in providing any care recommended by an MD who is more experienced in [at the sharpest edge of] PV treatment.
As I may have mentioned elsewhere [or above], we've had a good rapport from the start, and even though the nearest MPN 'super-specialist' [MPNSS from henceforth] acknowledged [by MPN Voice, IIRC] in my part of the country isn't that far away [at Roswell Park in Buffalo, NY], I don't want to ditch my MD to go that relatively short distance to see her [the RP MD].
My MD just [since Wed.] sent the MPNSS a referral letter introducing her to the particulars of my case, and my SWMBO is going to call 1st thing Monday AM to arrange a consultation appointment.
As a result, I think it will not be too awfully much longer before I climb aboard the Besremi treatment bandwagon- God willing, and the creek don't rise.
Thanks for your interest, advice, and good thoughts!
It is good to have that kind rapport with your MD. Even though she has limited knowledge of MPN, you can provide her with what you have researched about; and you hope something good would come out of that patient to provider synergy.
I chose a large network of doctors in my area after moving from California, the first hem I had was like that MD you have. He recommended that I consult the teaching doctor/university-based within the network who specialized in MPN - at least once a year. He said he can help in the maintenance of medication that is already proving to work for me based on what I can work with the university-based doctor.
I have stuck with the teaching MD and did not come back to the first hem. I think things are working just fine.
Whatever works best for you is the best thing to do- it's your life and health in the end.
My general hem/onc wanted me to see the 'MPN' specialist in her health system, but even on the health system's website, he didn't have anything that demonstrated his expertise- no published research, no statements of special interest, nada, so L'm going elsewhere- which she was still OK with.
This is a long and convoluted report that I found while looking for a different article, which I think it has some interesting points to add- to our discussion.
It especially supports not taking a wait and see [e.g., ASA and Phlebotomy-only] approach in early disease/low risk MPN cases:
The 2nd report I think is a mathematical exercise to correlate clinical results. The study it used was for 5 years. But if this plot is based on real data, it's a nice reassurance compared to another study I've posted on that shows MR past 5 years is conditional.
I also found this, which again is a [as are so many] somewhat complicated discussion, which to me boils down to interferon works in PV and ET - especially at preventing progression to MF or CML:Title:
Histomorphological responses after therapy with pegylated interferon α-2a in patients with essential thrombocythemia (ET)
I posted this one recently too, it is a good ref. One takaway is BMR (marrow response) requires at least 4 years, so it needs more patience than MR (Allele reductions) . Response typically lasts 2-4 years, this is surprisingly short. But some went longer.
"In the present study, we reported that AECAs exist in the sera of patients with PV and that AECAs are linked to thrombosis.
Therefore, we think that the measurement of AECAs in PV patients could
be recommended, particularly in those that still have thrombosis following cyto-reductive and antiplatelet treatment.
Statins are potent anti-inflammatory agents that also show a synergistic effect with JAK inhibition. Therefore, a role of statins in association with JAK2/1 inhibitors could be envisaged in future PV treatment."
<<Antiendothelial cell antibodies (AECAs) are commonly detectable in diseases associated with vascular injury>>
My take is the AECA is an effect in the correlation since thrombosis is associated with vascular injury and not special to MPN nor high AB. If so AB may be the more familiar driving issue. A way to check could be to track AECA in INF patients that get large AB reductions.
Their cohort had a high thrombosis rate, and had only phlb for cytoreduction. I don't think we see that with HU or INF. A related item, as in recent posts, the Cornell group found Phlb led to higher rates of progression than HU or INF, and progression can relate to inflammation etc.
So this article could be a small sample of reasons to not use Phlb exclusively.
-Sort of strange note on statins, it has been discussed in other reports, but they don't give it context.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")