I’m a 23 year old, healthy weight female. I’ve been struggling with my health for the last 5 to 6 years now.
I have a big long list of symptoms but most challenging are: extreme fatigue, joint pain (boney nodules on fingers, hot burning knees), Right Upper Quadrant Pain, brain fog, cold intolerance, hair loss, chest pain (struggle to take a full breathe in), heart palpitations and high heart rate (145 after walking up one flight of stairs at home, over 205 when exercising).
I have been tested for Thyroid Disorder at GPs, they concluded it’s not thyroid related.
I have this week been tested for Lupus via an ANA test - results are negative.
I know I should feel happy for results to come back negative, but I just feel I’m back at square one, with debilitating symptoms not being listened to and without a diagnosis.
Could I still have lupus??
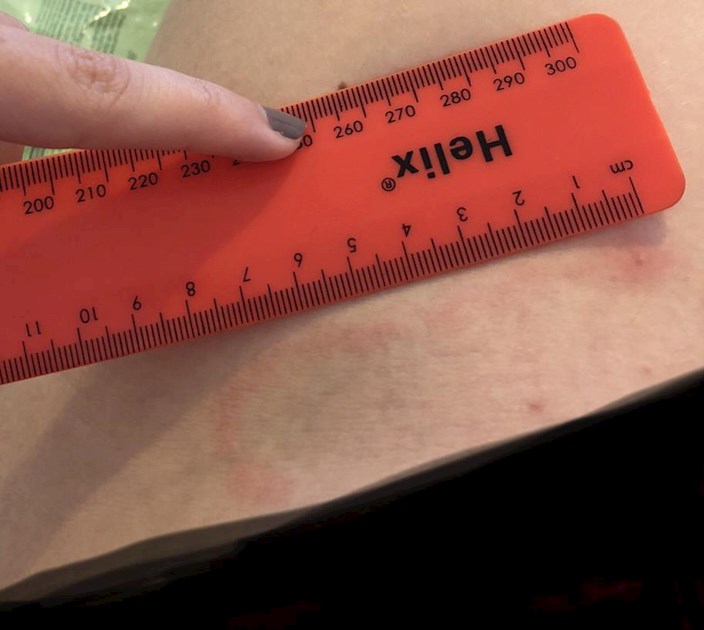
Back in May 2018, I had this rash appear on my leg, at the time I was naive and thought it was strange but didn’t got to the doctors.
Could this be a symptom of lupus? I have seen only one similar saying it is a sign on another website.
I would be massively appreciative of any advice on where to go from here? Suggestions of other tests or conditions would be really helpful!
Thanks so much!
Written by
M0lly
To view profiles and participate in discussions please or .
Welcome to the LUPUS UK HealthUnlocked community, we offer a free information pack which you can download or request at lupusuk.org.uk/request-info...
I'm sorry to hear you've been dealing with these symptoms for several years and I can understand your reasoning for not being happy despite receiving a negative ANA result.
An ANA test only confirms whether or not a person has an autoimmune disorder, it does not confirm if a person has lupus.
A dsDNA test is very specific for lupus. If someone tests positive for these antibodies, it often means they have lupus. To learn more about the specific tests and criteria needed to make a diagnosis of lupus, read our blog article at lupusuk.org.uk/getting-diag...
Many of the symptoms you have listed such as extreme fatigue, joint pain, brain fog, and hair loss are associated with lupus. We published a range of factsheets that discuss lupus and these symptoms which you may find helpful to read at lupusuk.org.uk/publications/
You may it helpful to take an information pack with you to your GP surgery when requesting a test for lupus. Please keep us updated, wishing you all the best!
A positive ANA by itself does not indicate presence of an autoimmune disorder. Presence of an antibody indicates autoimmune disease, although you could be seronegative and still have some autoimmune diseases. Some people with autoimmune diseases have positive ANA's, but not all individuals with autoimmune disease have positive ANA's. Some healthy individuals can have a positive ANA, and some medications cause a positive ANA. Autoimmune diseases are inflammatory, so inflammatory markers are routinely tested in people with autoimmune disease. SED rate (ESR) is a commonly tested inflammatory marker. A person with an autoimmune disease can have inflammation, but they don't always have a positive SED rate (ESR). CRP is another commonly tested inflammatory marker. A less known inflammatory marker is TNF-A, tumor necrosis factor alpha. Some people with autoimmune disease, have obvious inflammation, but they have completely normal SED, CRP, TNF-A. These inflammatory markers are not specific to autoimmune disease, they just measure inflammation in the body.
Hi MOlly, I’m so sorry to hear what you are going through, and at such a young age. If you read up on the ANA you’ll see there are false positives and false negatives. I think I had one negative amidst my positives🤷🏻♀️Idk why that is. Do you have a follow up appt? Usually they will do several more ANA tests on you (at least here in the US). I think they look for 3 positive ANAs before/while moving on to other tests, but you definitely have something going on with you, so you need to keep being seen. Lupus is called the great imitator. You definitely sound like you may have Lupus, but it could be UDCT/Latent Lupus, or something else related? So please keep seeing your doctors and figure it out. For some of us, a diagnosis took years of testing, so sit back, you may be in for a long journey, but you’ll get there. Be patient and keep us posted. Keep your attitude positive, as a positive attitude will help see you through. It may feel like a lot to face, but you’ve got this! 👍You can do it!!
Other related diseases that can cause these symptoms can be seronegative ie not show up in the blood for a percentage of sufferers. About 25% of people with Sjögren’s have normal blood markers but still get photo sensitive rashes, severe fatigue, hair loss and pain. If you don’t feel that your GP is aware enough of seronegative rheumatic diseases then it would be worth trying another with this and other photos and requesting a copy of your full blood count, inflammation markers etc. It can take a long time for people to be diagnosed with autoimmune diseases, especially if bloods are normal.
At least here in the US, I think they look for a few positive ANA’s while, perhaps doing other testing, before they move on to more in-depth tests like the
Anti-ds, and others. This is my belief, I could be very wrong.
Not necessarily. Proactive doctors will go right in for testing antibodies and specific tests. ANA is a general test. If positive, by itself does not indicate any specific disease, nor an autoimmune disease. Some healthy people have positive ANA's, some medications cause a positive ANA, and many people with autoimmune diseases do not have positive ANA's.
I understand that, that’s why I said they generally want to see several positive ANA’s but will sometimes do other testing along side it before they move on to more in-depth testing. I think you’re basically repeating what I said? Perhaps you misunderstood my intent? Bottomline, there are so many similar AIs to Lupus, any professional knows to be careful with a diagnosis. They won’t want to mistreat you by mislabeling.
Hi Brooksidecourt. What I wrote is not at all like what you said. Doctors do not wait around for several positive ANA's before they'll test antibodies or other specific tests. ANA is just one of many general tests that is used to help gather more information in a quest to make a diagnosis. It is not definitive of any specific diagnosis. Many people with autoimmune diseases do not ever acquire a positive ANA. Healthy individuals can have positive ANA. Some medications cause a positive ANA. It would be unprofessional for a "professional" to wait around for years for a positive ANA that may never show up before they'd test other specific tests. That would like be waiting for Godot in many autoimmune cases.
Ok, I’m not trying to argue with you. I’m assuming you are in the US? As am I. Yes, further testing but not all at once. I still say the in-depth testing comes along after they have a suspicion of a stronger case of AI, like Lupus, etc. Like miccika1 says here, Lupus is called ‘The Great Imitator’. It would be just as ridiculous for a doctor to pull out the big guns immediately, as it would for a doctor to start you on methotrexate the minute you show your first positive ANA. It just doesn’t happen.
Hi Brooksidecourt. Thanks. Me neither. Yes, I am too. There is no limit to how many tests are ordered at once. Process of elimination in ordering tests onesy-twosy style can save a patient money at the time, can draw out diagnosis and prolong suffering, so in the end wastes a patient's money (time and loss of live being undiagnosed is expensive). If a doctor is proactive, multiple specific tests will be conducted at the same time. Diagnosis is usually process of elimination until you run the right diagnostics and they eventually eventually come back with evidence of disease.
A positive ANA does not warrant for starting methotrexate or any other medication because positive ANA does not mean anything specific. Positive antibodies and other disease-specific tests would, however.
Remember, not everyone with Lupus has a positive ANA.
Lupus is a great imitator. Those symptoms could be lupus but also many other conditions. Keep searching and working with doctors to see what you have or don't have. Finally you could always try some therapies and see if it helps or not.
Hi Molly. I'm so sorry to hear that you have been suffering for so long without any resolution. Your symptoms sound very much like they could be thyroid disease, possibly Hashimoto's. Or you could have some other autoimmune disease. The rash on your leg: do you still have it or did it go away back in 2018?
What does "Thyroid Disorder" that you were tested for mean and what were the tests that they used to test for it? There is no general thyroid disorder. There is hypothyroidism, hyperthyroidism, Hasimoto's and Graves Disease. The last two are autoimmune diseases. Can you share what thyroid labs were done, the lab ranges and your results? If your doctor did not test the right thyroid disease labs, which is commonly how it goes, they cannot conclude that you don't have a thyroid disease. A lot of doctors get very confused as to which tests to run together and most don't know what the test and lab results mean, so they misinterpret the results. In order to rule out thyroid disease, you'd have to test the following: TSH, Free T4, Free T3, TPO/ab, TG/ab and Reverse T3. The first 5 are the most important. The 6th is the least important the first time testing. RT3 will confuse a typical doctor because an easy formula must be calculated between your FT3 and RT3 to arrive at the RT3 Ration, which is what matters. The two labs that matter the most are Free T4 and Free T3. If your results are not a least 50% of the lab range, you might have a thyroid disorder. If your FT4 and FT3 are at the top of range, you probably have a thyroid disorder. TPO/ab and TG/ab are antibodies to determine if you have autoimmune disease. Both of these have to be tested, not just one, in order to rule out autoimmune disease. TSH is a messenger hormone that comes from your pituitary gland and communicates with your thyroid. TSH is not a thyroid hormone and is not an adequate marker to evaluate thyroid function without the presence of FT4 and FT3 lab results.
Hi Molly. Sorry to hear that you have been suffering so much. Reading the posts here, it seems you have a sound steer in what to ask your doctors to follow up on next. You might also want to consider asking your doctors to rule-out vasculitis, or a vasculitis syndrome, which can present alongside other autoimmune disorders such as lupus and rheumatoid arthritis, or as a discrete condition in itself. I think in the UK at least it will be hospital doctors, such as a rheumatologist or immunologist, who can run these tests as G.Ps can't order them. So, push for a referral. Resist being written-off with a diagnosis of fibromyalgia or M.E. or CFS until absolutely everything else has been thoroughly tested for, and re-tested for at later intervals of time. That happened to me and only very recently was I diagnosed with urticarial vasculitis syndrome (a lupus-like syndrome - see vasculitis.org.uk for information generally). There's no test available yet for M.E or fibromyalgia, and logically everything else needs to be ruled out first before such a diagnosis is made. Notably, the difference in these diagnosis means that I have drug treatment now offered to me as opposed to being told to repeat CBT and graded exercise, which only ever made me feel worse anyway. Stay strong and confident that you know your own body best and know when it is physically sick. I wish you good luck on your journey.
Hi Molly I totally agree with you I was fortunate enough I had many tests and paid privately in the end as I was so unwell so everything else was ruled out they tested me for lupus and God knows what other stuff so mine genuinely was CFS had it for 15 years absolute nightmare left me with lung disease also and that’s still a nightmare but the CFS is in good remission🙏
I'm so glad your CFS is in remission. I hope that your lung disease is now also well controlled. Many of us seem to struggle for a very long time before we get proper answers. I'm so grateful for this forum as at times it's easy to slip into a mindset where I think it's only me that it's happening to! Clearly that isn't the case. Best wishes all.
Hi Sue_petal. These are not street acronyms. They are the actual names of used by laboratories for these blood tests. The full names are not typically spelled out but occasionally you might see a lab spelling a complete word here and there. These exact names are used by most labs.
Thyroid Stimulating Hormone (TSH) - TSH is a hormone that comes from your pituitary gland, not your thyroid. It is a messenger hormone that sends a message to your thyroid telling it how much hormone to produce, or how much not to produce.
Free Thyroxine (FT4) - FT4 is one of two thyroid hormones that regulate metabolism. T4 is main thyroid hormone and it is the pre-cursor to T3. However, it's T3 that has the biggest responsibility in regulating metabolism.
Free Triiodothyronine (FT3) - FT3 is one of two thyroid hormones that regulate metabolism. T3 is the active hormone, meaning it is more metabolically active than T4. T3 levels influence metabolism, energy levels, digestion and body temperature. T3 is also 5 times more potent than T4. T3 is produced whenT4 is converted into T3 by an enzyme. This conversion mainly happens in the liver. If you have conversion problems and have low T3, metabolic rate will not increase and metabolism will be slow.
Thyroid Peroxidase Antibody, or anti-Thyroid Peroxidase (TPO/ab) - Thyroid Peroxidase is a thyroid enzyme that is used to create T4. Antibodies against Thyroid Peroxidase are an autoimmune reaction that inhibits or reduces production of T4, leading to autoimmune hypothyroidism, Hashimoto's. Positive TPO/ab can also be present in people with Grave's Disease, autoimmune hypothyroidism.
Thyroglobulin Antibody, or anti-Thyroglobulin - Thyrogloblulin is a protein produced by thyroid cells and is involved in thyroid hormone synthesis. Antibodies against Thyroglobulin are an autoimmune reaction that causes dysfunction in thyroid hormone production. TG/ab can be present in both thyroid autoimmune diseases, Hashimoto's and Graves Disease.
Reverse Triiodothyronine (RT3) - RT3 is an inactive thyroid hormone. In excess or in poor ratio with current levels of T3, RT3 can bind with thyroid receptors. When this happens RT3 prevents T3 from getting into cells, which in turn lowers metabolism. Determining the cause of high RT3, or a bad RT3/FT3 Ratio (under 20) and why T3 is not getting into cells can help correct the problem. Low iron, D3, selenium, zinc, B12 and B6 can cause poor RT3 Ratio. Also high antibodies (need to determine what is triggering antibodies to increase and remove that trigger), exposure to toxins, illness, stress, leptin resistance, too high or too low cortisol, insulin resistance and diabetes, infections, and liver issues (thyroid hormone conversion happens mainly in the liver).
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

") Yes, I am too. There is no limit to how many tests are ordered at once. Process of elimination in ordering tests onesy-twosy style can save a patient money at the time, can draw out diagnosis and prolong suffering, so in the end wastes a patient's money (time and loss of live being undiagnosed is expensive). If a doctor is proactive, multiple specific tests will be conducted at the same time. Diagnosis is usually process of elimination until you run the right diagnostics and they eventually eventually come back with evidence of disease.
Yes, I am too. There is no limit to how many tests are ordered at once. Process of elimination in ordering tests onesy-twosy style can save a patient money at the time, can draw out diagnosis and prolong suffering, so in the end wastes a patient's money (time and loss of live being undiagnosed is expensive). If a doctor is proactive, multiple specific tests will be conducted at the same time. Diagnosis is usually process of elimination until you run the right diagnostics and they eventually eventually come back with evidence of disease.