hi just a quick question if anyone has any more info on this will be much appreciated
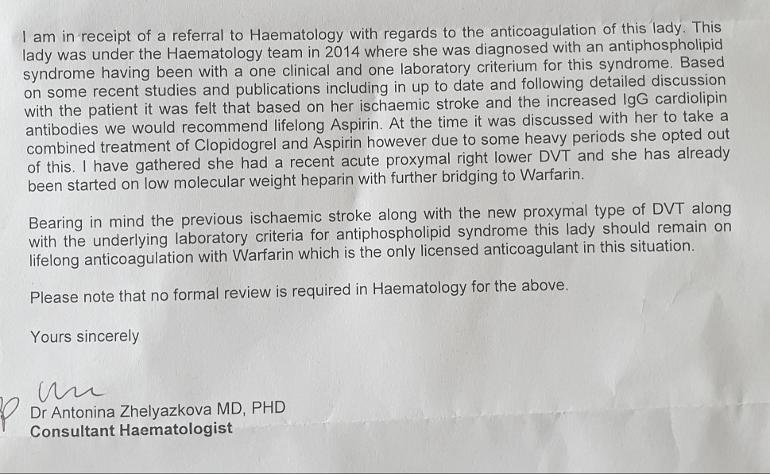
so I have just received a letter from haematology. I will attach
little bit confused as its such along time ago and only ever seen this lady once. I don't ever remember been asked to take asprin but then again I just had a stroke and remembering wasn't my best freind then. Just asked the hubby he said the same he doesn't remember that.
anyway is it normal when you have APS to not have to go a see someone if your already on warfarin. And is that it . Just a bit confused with it really
My understanding of that letter is that they are saying that you don’t need a review at the Heamatology Clinic because as far as she’s concerned she’s got all your history and feels that you need to be on life time warfarin which is the standard treatment for APS especially as you have clotted again. Have they given you a target INR and who will be monitoring it?
If your still unhappy about not being seen in the clinic you must ask your Gp to refer you to an APS specialist like Prof Bruce. He may put you on other medication such as Hydroxychloroquine.
Thank you for that makes sense . am going to see if I can get a referral from the gp to to professor Bruce cheers. INR target been told between 2 and 3 from the anticoagulant nurse . I'm not to sure who monitors it would this be the nurse.
Probably however she may not understand that people with APS often have to have an INR of 3-3.5. The 2-3 you quote is a bog standard for people with other conditions and is often not high enough especially if you have re-clotted. Another reason to be under a specialist.
Thanks for this information ive just been discussing this with husband. and looking back with him. I had my stroke seen her straight after had no issues regarding history to tell her apart from stroke 2 normal births and thats it. All my symptoms came after this and I just put it all down to the stroke b12 and constant anemia and my brain just not working right and got on with it but over the years things have got worse. So I definitely think I need seeing again to properly go through whats been happening . Thanks for that with the INR I didn't know this.
Worth noting that I think this patient is in the UK where British Haem Soc guidelines clearly state that: "The target INR for VKA therapy in APS should normally be 2·5".
Now, that might be controversial in this group, and I know there are specialists (even here) who disagree, but actually even in the international APS task force guidelines there is no strong recommendation on range following ischemic stroke (the only one is vague, and un-graded due to no consensus among specialists), and following venous clotting the international recommendation is 2-3. I think the only UK guideline for >3 INR for APS is if you have clotted through 2-3 (when in range) - which the poster does not seem to have done.
So, I suspect the Haem clearly understands the guidelines she is working under and doesn't want to put her arse on the line by going outside of them. I would also personally venture to suggest that it might actually be a teeny bit silly to put a patient straight on INR 3-4 when they have previously discontinued anti-platelet therapy due to bleeding. Anti-coagulation is always a balance between clotting and bleeding risks.
My own experience: ischemic stroke, LA +ve, recommended anti-platelets by one consultant, warfarin at 3-4 by one consultant and warfarin at 2-3 by multiple other consultants. Currently on warfarin 2-3 with no recurrence in 7 yrs. Actually never felt well on warfarin, wish I'd stayed on anti-platelets, wish I felt as well as I did back then.
“I would also personally venture to suggest that it might actually be a teeny bit silly to put a patient straight on INR 3-4 when they have previously discontinued anti-platelet therapy due to bleeding.”
I was not aware from anything in Hidden post that indicated any bleeding events?
Letter states that anti-platelets were discontinued due to "heavy periods", that generally means bleeding...
How "heavy", how much bleeding, is anyone's guess - we tend to be really bad at estimating blood loss, take a quick search at how many blood-loss-estimation charts there are and you'll realise that even the pros are notoriously bad at it.
"Heavy periods" is defined medically in some places as >80ml blood loss, a typical sanitary pad holds 5ml, that's five ml, a teaspoon. I admit I used to joke about my wife bleeding "like a stuck pig", usually when cold-salt-soaking another set of sheets with dinner-plate sized bloodstains - but I knew it was a joke (one I am paying for now in karma - how I wish I was back in those days), in reality it was probably a few ml of blood. Blood goes a long long way.
Blood donations are given in pints, apparently without problems, yet "heavy periods" can definitely cause medically significant problems like anemia. Significant enough to take a patient off prophylactic anti-platelets? - well with hindsight clearly not, but you can't prescribe with hindsight.
It should be a Doctor who prescribes Warfarin. I can tell you I have an INR range between 3.5 - 4.0 and have taken warfarin since 2012. I live in Sweden and selftest as I want to know that I am in range all the time. That is exstremely important when we have Sticky Blood and to have a Specialist also of course. I do not know how many of the 3 different antibodies they have taken on you to get a diagnose. I am positive to all three with high titres all the time, but you can be positive to only one antibody to get a diagnose of APS if you also have had symptoms typical for APS.
Try to learn as much as you can about this tricky illness that so few Doctors know. A good book is "Sticky Blood Explained" by Kay Thackray. She has APS herself and prof Graham Hughes has told us also that it is one of the best books that has been written about our illness. I have several books written by the Prof himself also.
Hi, as mentioned above, those with Hughes Syndrome/APS usually need to carry a higher INR, this must be set up carefully by the prescribing consultant who should have a working knowledge of this condition. I a sure you can book a phone call if you ring up to express any concerns you have. MaryF
Hi, I am turning off replying to this post as it looks like the member has left.If anyone wants to continue this subject please start a new post thanks.
The ability to reply to this post has been turned off.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.