It seems most major research about Adaptive Theory (AT) applied to PCa is now coming from Dr. Robert Gatenby, Co-Director, Center of Excellence for Evolutionary Therapy at the Moffitt Cancer Center in Tampa, FL. Here are two recent papers that attempt to lay the groundwork for mathematical models that could be used to formulate treatment programs for individual patients; i.e. are patient specific. And while the first model is not specifically based on AT, it would of necessity include and help define effective adaptive treatment regimes within the range of the model. Also included is a third paper from German researchers who look at AT as it relates specifically to the Androgen Receptor in PCa.
The first paper describes a conceptual mathematical framework for treatment models to be used by treatment boards in directing treatment programs for a particular patient. The second paper is an earlier one that is based on clinical results and likely informed the framework proposed in the first one. It specifically addresses AT (referred to in the paper as ‘evolutionary stable therapy’) when applied to the treatment of mCRPCa.
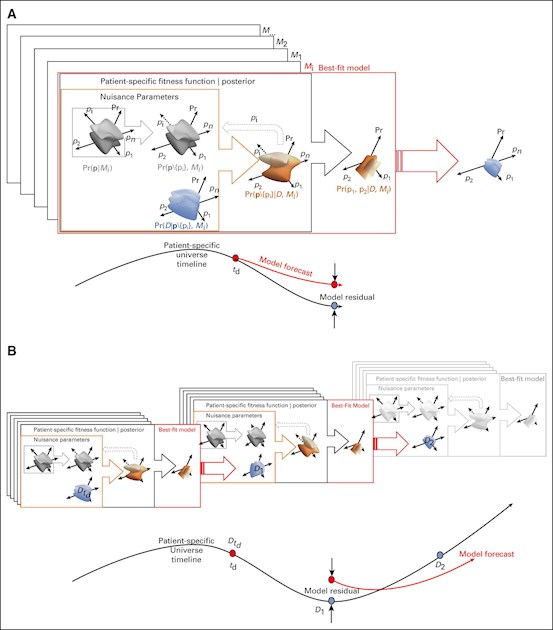
This first paper (co-authored by who else but our AT pioneer, Robert Gatenby) is extremely technical and definitely not for the mathematical-modeling novices among us. For those without any grounding in mathematical models or construction of algorithms, you may best skip the details sections and go to the Discussion section at the end. The first sentence in that section is:
"Here, we advanced the idea of a framework to support the decisional theory modeled on tumor boards' function to identify patient-specific clinical pathways."
The research team's "Key Objective" was:
"How to decide on the optimal treatment for a patient? Our approach aims to rate tumor-board-preselected optimal treatments with a Bayesian statistical tool rather than determine optimal treatment through externally specific indexes."
BTW, For those who are unfamilar with the term "Bayesian", here is what Merriam-Webster has to say about it:
Bayes·ian | \ ˈbā-zē-ən, -zhən \
Definition of Bayesian: being, relating to, or involving statistical methods that assign probabilities or distributions to events (such as rain tomorrow) or parameters (such as a population mean) based on experience or best guesses before experimentation and data collection and that apply Bayes' theorem to revise the probabilities and distributions after obtaining experimental data.
And here Wiki's page on Bayes' Theorem:
en.wikipedia.org/wiki/Bayes...
The first paper is here:
Bayesian Framework to Augment Tumor Board Decision Making - JCO Clinical Cancer Informatics - Published online: May 11, 2021
ascopubs.org/doi/10.1200/CC...
The second paper, also co-authored by Dr. Gatenby, will be of more specific interest to PCa patients, as it used treatment outcomes of patients treated with abiraterone and focuses on the concepts that underpin AT when applied to mCRPCa in the clinic. It is also technical in nature and likely well above the pay-grade for most readers here. It is a very thought-provoking paper, as it challenges the treat-to-failure/resistence SOC practice that is still in mainstream use for PCa today. This is from the Introduction:
"For instance, a type of evolutionary therapy known as adaptive therapy uses drug holidays timed specifically to each patients’ disease dynamics in an attempt to intentionally maintain a sufficient level of drug sensitive cells [8, 11–14]. Upon withdrawing therapy, these sensitive cells can compete with and suppress resistant cancer cells, thus prolonging drug efficacy. Continuous or maximum tolerated dose therapies quickly eliminate the entire sensitive population resulting in treatment failure as resistance cells can now grow unchecked. Adaptive therapy clinical trials are underway in multiple different cancers including trials in metastatic castrate-resistant prostate cancer (NCT02415621, NCT03511196), in melanoma—NCT03543969, and in thyroid—NCT03630120."
The full paper can be found here:
Optimal control to reach eco-evolutionary stability in metastatic castrate-resistant prostate cancer - PLOS ONE - Published: December 8, 2020
journals.plos.org/plosone/a...
And, finally, this review paper on AR adaptability supports the need to be more creative than is the traditional treat-continuously-to-CR/failure SOC model that has been used for a generation or more. This is from one of the paper's figures is key:
"In general, due to accumulation of mutations, a tumor is composed of many cancer cell types leading to tumor cell heterogeneity. Cancer consists also of cancer stem cells (stem) and other non-cancerous cells (other, including cancer -associated fibroblasts and immune cells). Androgen-deprivation therapy (ADT) is mostly successful inhibiting the growth of androgen-sensitive PCa cells. However, castration-resistant cells may be selected by the treatment and accumulate. Treatment with AR antagonists and other therapeutic drugs, including chemotherapy and radiation, might select for drug resistant PCa cells leading to a more aggressive tumor (such as NEPC). Associated with the tumor evolution, during tumorigenesis PCa develops a variety of androgen bypass signaling."
The authors also suggest that senescent cells may play a sort of stealth role in promoting tumorgenesis. They go on to offer that senolitic compounds (which are known to be able to eliminate/reduce senescent cells) may be a new treatment avenue. This is a very comprehensive paper on the mechanisms involved with the AR function in PCa and a good read for those that want to deep dive into AR.
The full report is available here:
Androgen Receptor-Dependent Mechanisms Mediating Drug Resistance in Prostate Cancer - Cancers (Basel) - 2021 Mar 26
ncbi.nlm.nih.gov/pmc/articl...
Much to consider as we all try to make decisions about the increasingly complex world of cancer treatment. I'm on a self-directed n=1 AT trial and am glad to be there. If I had gone the SOC route, I would surely be CR now and would have also had the QOL hit of ADT for the last 3 1/2 years. Dice roll, for sure - but so far, I'm way ahead at the AT gaming table. Chips Ahoy!
There is a short Part Three to follow in a few days. In the meantime, Stay Safe & Well - Capt'n K9
