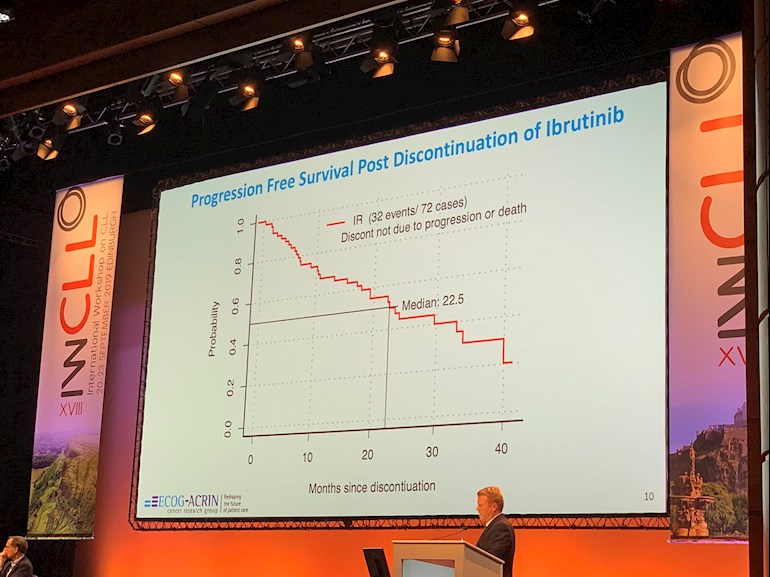
An update re the E1912 trial reported at iwCLL this year - "patients who stopped ibrutinib for toxicity had a median PFS from the time of stopping ibrutinib of about 2 years which is reassuring news. This phenomenon is in clinical practice, good to see similar data from a RCT. However, there is no information about how long patients were on Ibrutinib prior to stopping for toxicities."
More information about this study here: lymphomahub.com/medical-inf... Main take home message is that with the current follow-up, IR was also superior to FCR in IGHV unmutated patients but not in IGHV mutated patients.
Jackie
Written by
Jm954
Administrator
To view profiles and participate in discussions please or .
Interesting I wonder if patients even those like myself who are fine with ibrutinib and in remission could have treatment breaks as with the V+I trail and then restart treatment when needed which hopefully would help stop resistance from ibrutinib .
There is going to be a study in the UK where patients on Ibruitnib will be randmised to stop or continue Ibruitnib. The stop cohort will restart after 1 year or if CLL increases, whichever is soonest.
I would welcome stopping Ibrutinib if I knew it would respond again when restarted.
Many of the Ibrutinib patients in FLAIR could participate.
Yes same for me Jackie although there are new btk drugs on the way which could take up where ibrutinib fails it would be nice and cost saving to the NHS if we could have breaks safe in the knowledge that it will work just as well as from when we stopped
What is considered being in remission when taking ibrutinib? I didn’t really think that was possible. My doctor has not mentioned remission (neither as a status nor as a possibility.)
I had a different doctor ask me if I was in remission and I said I wasn’t, though my labs were getting better. (I figured if I was in remission, my oncologist would have said something.).
Venetoclax with an antiCD20, especially obintuzumab, is very very effective at giving people remissions so deep that no CLL can be found - so called U-MRD. Very rare to get that with Ibrutinib but deeper responses are found the longer people are treated with it.
TO REPEAT "Ibrutinib Rituximab/IR was also superior to FCR in IGHV unmutated patients but not in IGHV mutated patients."
Unfortunately, I have seen quite a few incorrect assertions by some members that IR is superior to FCR in all circumstances. Not only is this misinformation potentially dissuading members able to access IR and FCR from considering FCR, which has been shown to provide 60% of those with mutated IgVH with indefinite remissions approaching 20 years, it is also unnecessarily distressing members who live where it is impossible to access Ibrutinib.
Again - directly from the presentation, "With the current follow-up, IR was also superior to FCR in IGHV unmutated patients (HR = 0.26; [95% CI, 0.14−0.50]; P < 0.0001) but not in IGHV mutated patients(HR = 0.44; [95% CI, "0.14−0.136]; P = 0.07)
This 2015 paper documents the very long term progression free survival for IgHV mutated folk, with the plots B, C and D showing the statistically significantly superior results over unmutated IgHV folk: ncbi.nlm.nih.gov/pmc/articl...
Impressively, per plot D, about 80% of IgHV mutated folk that achieved MRD negative status on FCR treatment, saw no progression of their CLL in 15 years. Just 20% had remissions shorter than 7 years. In other words, the 80% that made it to 7 years without progressing remained progression free out to 15 years (and presumably 20 years now,)
So for the 50% of our membership that are igHV mutated, that's a pretty good investment return for 6 months treatment. No worries about developing resistance to a maintenance drug, atrial fibrillation, high blood pressure, financial toxicity or living with side effects. They can forget that they have had CLL. That's why some CLL specialists still recommend FCR, including specialists at M D Anderson. Not surprising considering the paper includes the well recognised specialists at or from M D Anderson, such as Philip A. Thompson, Constantine S. Tam, Susan M. O’Brien, William G. Wierda and Michael J. Keating. No treatment is risk free (which is why we still have Watch and Wait, so yes, those treated with FCR do have an increased risk of developing Myelodysplastic Syndrome (MDS) or Acute Myeloid Leukaemia (AML). I expect that eventually non-chemo treatments will replace chemoimmunotherapy, but we aren't there yet.
Thanks for this information Neil as someone who is about to start FCR I find these numbers encouraging. Being in Canada we do not have the same options as other countries (US in particular) and are limited in our First line Treatment choices unless you are 17p or Tp53. In addition to that each province has their own restrictions on what is funded.
That is one thing I would encourage members to be aware of when suggesting treatment choices for others in different parts of the world. It is what is in a Universal health care system unless you have deep pockets. Even with private insurance there is no guarantee they will cover other treatment options if you fall under the country's acceptable treatment guidelines.
My hope is when and if I relapse there will be so much better on the horizon!
Even though you record in your profile that you live in Canada (and I so wish everyone would show where they live in their profile or as a suffix to their username), I think even most Canadians would be very careful about suggesting treatment choices for the reasons you state.
We're from Canada. I think the point Red was making is that in Canada, access to ibrutinib and other medications is restricted because the health care system doesn't cover the exorbitant costs of these medications (although coverage is expanded in Ontario and other provinces). Patients should receive the medication that evidence has shown is safest and most effective for their condition.
Hi ikahan I believe that is the point Neil was making. He is from Australia where their frontline protocols are similar to ours as is the UK. Where I live there are no trials close by...again another restriction. We can only hope that in these countries we will have better access to treatments in the near future. Thanks for responding!
Thanks for your post. I am heading toward treatment and am fortunate to be under 65, IgHV mutated with no deletions of 17p 13q or 11q and no mutations in TP53, NOTCH1, SF3B1. In other words, an ideal candidate for FCR.
My oncologist suggested FCR, but I consulted a well known specialist recently who suggested Venetoclax plus Obinutuzumab. As you may know this a fixed-duration regimen (12 months) just recently approved by the FDA for first line. It is producing very strong remissions (better than FCR) but we do not know what the long-term prognosis is because there has not been sufficient time for follow up.
Some people seem to feel that it is better to avoid chemo altogether due to toxicity. I am aware that FCR increases the risk of severe and prolonged neutropenia, may damage DNA, and increases risk of MDS and AML. My oncologist also said there is 15% chance of Richter's transformation after FCR. This was news to me and I can't find much about that in the literature.
It is not clear if my insurance company will cover V+ O because it is substantially more expensive than FCR. On the other hand it is a lot cheaper than lifelong therapy on Ibrutinib.
I am conflicted about what to do. Should I push for the V+O (or enroll in a trial) or take the path of least resistance and "settle" for FCR because it is very likely to produce a long remission?
I might not be popular saying this but I personally would have V+O if there if I had the opportunity.
15% chance of Richter's sounds high with your genetic markers, that might be the cumulative risk over many years. Of course it's not know what it is with V+O yet.
From my understanding of IR vs FCR for mutated folks IR was slightly superior in all cases but not significantly so, it was practically a tie. Husband is 13q- and mutated and 44 and we jumped at the I+V+O trial and would have done V+O outside of a trial. The long term FCR numbers for mutated are great but MDS and secondary cancers are the known downside of FCR and the reason why many specialists in the US have moved away from it. Plenty of unknowns still with the newer drugs too for sure.
Thank you so much for this post Mldeterm. It gave me some reassurance. I was concerned and confused because my US CLL specialist doesn’t use FCR but I read above many very well known CLL specialists still do.
Grumpyfrog, I agree with Jackie about the 1 in 6 chance of developing Richter's sounding too high. If so, why aren't there many more reporting it here? I seem to recall the 15% being derived from early reports from patient trials where many of the trial participants had had quite a few prior treatments, with the most recent estimates around the 5% mark.
The future has to lie with combination non-chemo short term treatments, most likely Venetoclax and another synergistic drug or two to speed response while reducing the likelihood of resistance developing, thereby allowing future re-treatment if needed.
You are in the enviable situation of being able to choose between the current international gold standard with 20 years of data offering you a 60% chance of what's effectively a cure (80% if you achieve U-MRD) or perhaps the new gold standard. I'd be tempted by the V+O too. We need people to help us find better treatments.
From what I recall most RT percentage increases early on then the percentage of people who get it levels off. Dr. Furman mentions it in a couple videos uploaded to youtube. Lymphoma & Myeloma Congress?
I'd be interested in any references regarding changes in risk of RT over time. The 2 - 10% overall fits in with what I've seen more recently. We also know that the risk is higher with specific markers. I suspect the actual rate is difficult to pin down because of the low incidence (but still too high with challenging treatment prospects) in what's a rare cancer. Likewise determining the cause(s) is difficult, due to the challenges in teasing out what they could be from the varied previous histories. A research centre with access to blood samples taken over time from patients that developed RT could do some valuable research with the latest DNA analysis tools, trying to identify how precursor changes develop and what triggers them.
I find it tricky to interpret. So continuously a certain percentage of the population gets it every year? Or by year 4 most people who will transform have already. It is a CDF I think.
Great video by Dr Furman thanks, with the Richter's Transformation (RT) part of the presentation starting at 12:40, where he identifies the baseline risk factors for RT at 14:00. Dr Furman first points out that 46% of RT happens prior to treatment and that "Richters is really in the biology of CLL and not necessarily something treatment related". Surprising that the median time to developing RT is 1.8 years.
Well worth viewing by anyone concerned about where they fit with regard to the risk factors for RT.
Yes I agree, it's a Cumulative Distribution Function (CDF)
Interestingly Dr Lamanna said that the Richter's that she is seeing in patients who have been treated with novel agents (non chemo) are not as aggressive as those after chemo or before any treatment at all.
I'll look to see if I can find any references or more evidence for what she said.
My husband has the Notch 1 mutation he is also unmutated IGVH and CD 38 +. I have been very concerned about him getting RT. We looked at the original paper with the graph that shows that 45% of Notch 1 patients developed RT by 15 years ( 30% in the first 5 yrs ). However every single one of these patients has had FCR. So how was it determined that Notch 1 is an independent risk factor ?
Thanks. I was surprised and I thought the 15% figure was too high as well, which is why I was questioning it. I actually put up a new post today to see if anyone knows about this.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.