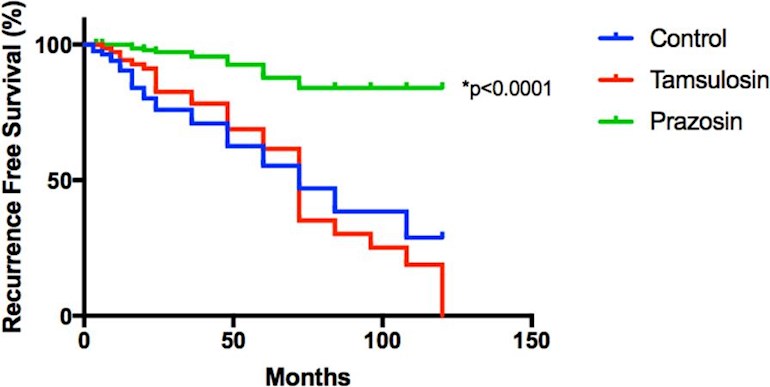
The sheer beauty of the retrospective study posted recently by Scout4answers is the vast superiority in Recurrence Free Survival for Prazosin users over a ten-year period not only against controls but against a similar drug, Tamsulosin. IMHO this means that selection bias is much less likely. Prazosin and Tamsuolosin are both used for lower urinary tract symptoms (LUTS) and high blood pressure. Both are α1- adrenoceptor antagonists but Prazosin is of a different subtype, quinazoline based, compared to Tamsulosin which is a sulphonamide derivative. These have some different characteristics which could account for their spectacularly different outcomes.
The adjacent graph posted by Scout4answers shows the most beautiful one I have seen in a long time.
What was left unanswered in the thread on Prazosin, reported on earlier by Patrick/Pjoshea 13, is the dosage and duration of Prazosin use to aim for if one wants to try this drug.
I had a telephone conversation with Professor David Christie, lead researcher in the ongoing prospective study on Prazosin, and a co-author of the retrospective study. My question was why the new study is using up to 10 mg prazosin daily, i.e. within the typical range used for high blood pressure, vs the 1-2 mg daily used of Prazosin in the first study, by patients with LUTS where lower doses are used.
His answer was that it is hard to translate the doses used in the preclinical trials to humans and that the hope is that the higher doses will prove to be even more effective than that indicated by the lower doses, even for the short time that the new study entails.
I asked him why the prospective study will only medicate with Prazosin for six weeks, vs 3- 5 months use in the retrospective study. His answer was that the new study, although progression free survival and PSA kinetics will be measured, is primarily a feasibility study to help guide development of a large-scale clinical trial for use of Prazosin by men undergoing radiotherapy for prostate cancer. Caution is used since there may be toxicity using Prazosin for prostate cancer patients without high blood pressure who are included in the study (men lower than 100/70 will be excluded).
My take is to start low with 0.5 mg avoiding hypotension, then slowly increase until 10 mg, or lower if there are noticeable side effects. If side effects don´t show up, I may aim for 3 – 5 months, as per the first study, before tentatively stopping for a considerable time to avoid risk of loss of efficacy. “Results (from Prazosin use) are rapid and can generally be evaluated by 4 weeks. When used for more than two years, prazosin becomes less effective and higher doses may be required. This may be due to tachyphylaxis (progressive decrease in response to a given dose after repetitive administration), or a progressive increase in prostatic size which is not influenced by prazosin's effects on muscle tone”.
“The most important adverse effect is postural hypotension, but stuffy nose, headache and retrograde ejaculation may also occur”. Hypotension = blood pressure under 90/60, often with no symptoms, but dizziness, fainting can occur.
The first, retrospective study linked by Scout4answers
nature.com/articles/s41598- ...
The newer prospective study anzctr.org.au/ACTRN12621000...
Any input from (potential) Prazosin users?

")