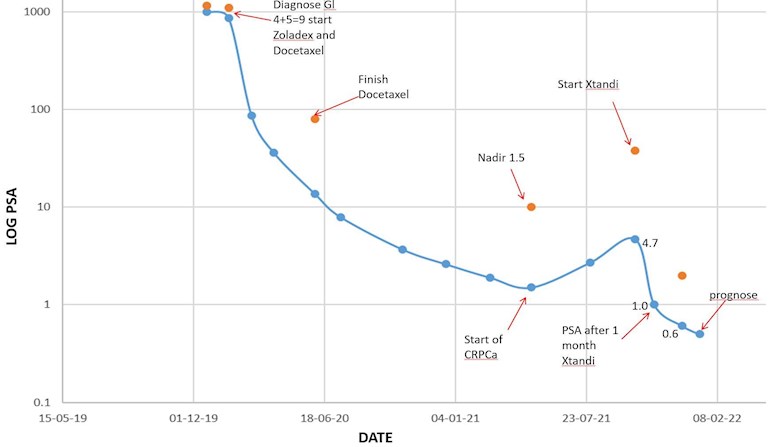
I am looking to the next step. As you can see summarized in the Log plot I have been through Docetaxel (SOC 6 sessions) with ADT (Zoladex) which I am still on. I have a cancer type which gives a large PSA response as you can see. Became castrate resistant in may 2021 and went on to Xtandi in October. Seems to be working though I suspect that my coming nadir will be over 0.1 – which doesn’t worry me since I still have a prostrate. My oncologist says the the next step is chemo when Xtandi stops working. My next meeting with him is early February and I am looking at the options to discuss with him.
My question to the forum is –
is it worth doing a single session of chemo now before Xtandi stops working – zap the enemy while he is weakest?? – anybody read anything about that – or experienced that? I read that 50mg Docetaxel every two weeks was better than 75mg every three weeks – which I interpret as that smaller doses are still effective but less destructive.
Second – should I go back on Docetaxel when Xtandi fails – or is it better to use LU-177 or Cabazitaxel next time around?
Any ideas??
Written by
Stoneartist
To view profiles and participate in discussions please or .
I don't think you are castrate resistant. You seem to be responding well to xtandi. You have not mentioned any other ADT drugs, i.e, zytiga, etc that you could go to "if" xtandi failed.
If any bone mets begin to increase, you might consider adding Xofigo to xtandi.
I reckoned I was castrate resistant because the PSA downward curve was abruptly broken by an upward curve. And yes Xtandi seems to have immediately reversed this trend. Isnt this typical for castrate resistance??? - thats what the oncologist reckoned as well???
I only have one comment. Your MO indicating going to chemo when Xtandi fails is possibly and you may know already this ...the use of chemo in that case to re-sensitise your cells so that either Zytiga or Xtandi will be effective again. From my anecdotal experience Cabazitaxel seems to be used when chemo is instituted for a second time.
Hitting it hard while it is weak. Yes. My mind wanders in that direction but cell behaviour being so complex it is difficult to know if my layman's mind to kill as much of this as possible is overpowering scientific research that contraindicates it.
Hopefully more will respond here.
A couple months ago Mateo Beach had a good post on Extinction Vortex which falls into what you and i think about.....Hit it hard some more now that we have a low PSA and greatly reduced met activity.
The definition castrate resistant means that your PSA will no longer respond to ADT treatments. Just because xtandi fails does mean that zytiga or another ADT drug would not work. Castrate resistant means your PSA would still rise even with a low testosterone reading.
Based on what my doctor has said, I think rechallenging Docetaxel or going to LU-177 are both good options when Xtandi becomes ineffective. Regarding Docetaxel, my doctor said "If there's something there, you go back to the well." In my case, my PSA rose within 6 months and he said he didn't think going back to Docetaxel would be a good option for me.
In your case, your PSA stayed down for quite a bit longer after you stopped Docetaxel so might be worth going back to it. You can always switch to Cabazitaxel if it's ineffective.
In the meantime, you could find out (when you get closer) if you have good PSMA expression and therefore a good candidate for LU-177.
My doctor told me he would recommend LU-177 before chemo for me, although it's still not approved in the US so I'd have to travel and pay out of pocket right now.
(1) The problem with adding chemo while Xtandi is still working, is that the chemo doesn't work. Chemo only works on rapidly dividing cells. Cells that survive Xtandi, survive by going into a dormant state. While dormant, they are not susceptible to be killed by chemo. You have to wait until PSA has risen significantly, or metastases increase.
(2) Lu177PSMA617 is best for your next therapy according to this:
From the article: The authors concluded that despite the advanced disease type of the subjects in this study, cabazitaxel plus enzalutamide was a tolerant combination and showed promising antitumor activity, particularly in abiraterone-naive patients. More data is needed regarding this combination therapy before any recommendations can be made.
Preclinical data suggest enhanced efficacy of cabazitaxel when combined with hormonal therapies for metastatic castration-resistant prostate cancer (mCRPC). Clinical studies on combining taxanes, i.e., docetaxel and cabazitaxel, and AR-targeted agents, that is, enzalutamide and abiraterone, are ongoing.
Oh yes. There may be a very good idea to do a taxane chemotherapy exactly when you are at nadir. This is the principle of “first strike/ second strike” that is the Extinction Dynamics approach for attempting cure. See my posts on this topic as well as those of Nal. You have to change treatments up before they fail, and preferably “when it is weakest” as you point out. For some reason this has not been incorporated into routine PC practice, even though it is widely used for other cancers with great success.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.