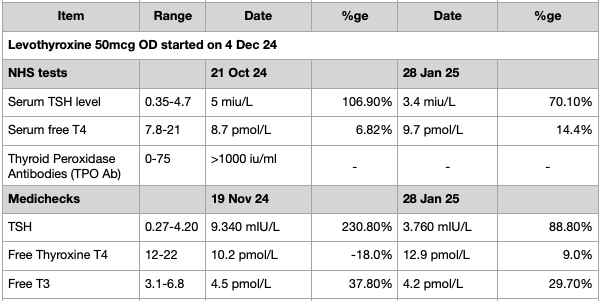
Routine blood tests on 21 Oct 24, following a PET-CT scan showing a hot area in my thyroid, showed significantly elevated thyroid antibodies but normal T4 and only slightly elevated TSH. GP was advised by Endocrinology that If my TFT showed subclinical hypothyroidism then GP to follow NICE Guideline [NG145] Thyroid disease: assessment and management Section 1.5 (Managing and monitoring subclinical hypothyroidism)
TSH was above the reference range (but just lower than the 10 mlU/litre threshold) on NHS test of 21 Oct 24 and private test on 19 Nov 24. GP agreed to a 50mcg trial for 3-6 months, to continue if symptoms improve, with testing every 6-12 months. Surgery pharmacist agreed to revise testing to every 8 weeks as 6-12 months too long.
I have felt much better since taking Levothyroxine with improvement in symptoms. I have booked a review with the GP next week and just wanting to make sure I understand what I should be asking for as next steps. It was heavy going to get GP to agree to trial in first place.
I had an NHS and private Medichecks test on 28 Jan 25 (~8 weeks) to see where things are at. Both used the same veinous sample, tested at 0910hrs, Super B-Complex stopped 7 days earlier and tested 24 hours after last Levothyroxine dose. I am male, 64 and 117kg.
Test results are as attached but I am unsure what this is telling me. From latest results it seems TSH is now within reference range from both the NHS and Medichecks test on 28 Jan 25. GP has noted in NHS test results “Normal, no further action required”. Does this mean that 50mcg is the correct dose? Or that I have to wait a further 4 months until the trial ends (and then what?).
Para 1.5.4 of NICE [NG145] says:
1.5.4
Consider a 6-month trial of levothyroxine for adults under 65 with subclinical hypothyroidism who have:
* a TSH above the reference range but lower than 10 mlU/litre on 2 separate occasions 3 months apart, and
* symptoms of hypothyroidism. If symptoms do not improve after starting levothyroxine, re-measure TSH and if the level remains raised, adjust the dose. If symptoms persist when serum TSH is within the reference range, consider stopping levothyroxine and follow the recommendations on monitoring untreated subclinical hypothyroidism and monitoring after stopping treatment.
I do not understand at what point in the trial does sub-clinical hypothyroidism become confirmed as primary hypothypoidism and, hence, subject to dosage based on weight? Do I just continue indefinitely on 50mcg until such time as the Hashimoto’s damage means TSH levels rise to over the 10 mlU/litre threshold on a NHS TSH test?
Many thanks for any advice.
Written by
Flamborian
To view profiles and participate in discussions please or .
Results show you are ready for next increase in dose Levo up to 75mcg
Which brand of levothyroxine are you currently taking
Try to remain on same brand as dose increases (only change one thing at a time)
Retest again in a further 2-3 months
Guidelines of dose Levo by weight
approx how much do you weigh in kilo
Even if we frequently start on only 50mcg, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or somewhere near full replacement dose (typically 1.6mcg levothyroxine per kilo of your weight per day)
Adults usually start with a dose between 50 micrograms and 100 micrograms taken once a day. This may be increased gradually over a few weeks to between 100 micrograms and 200 micrograms taken once a day.
Some people need a bit less than guidelines, some a bit more
If symptoms of hypothyroidism persist despite normalisation of TSH, the dose of levothyroxine can be titrated further to place the TSH in the lower part of the reference range or even slightly below (i.e., TSH: 0.1–2.0 mU/L), but avoiding TSH < 0.1 mU/L. Use of alternate day dosing of different levothyroxine strengths may be needed to achieve this (e.g., 100 mcg for 4 days; 125 mcg for 3 days weekly).
Many thanks SlowDragon for the quick reply. I am on Accord, but think I may have read they don't do 25mcg doses. I understand the dosage by weight issue when it is conformed as primary hypothyroidism. What is not clear is at what point in a sub-clinical hypothyroidism trial does dosage by weight kick in? The NICE Guideline appears totally silent on the issue if I understand it correctly.
Hashimoto's affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function can lead leaky gut (literally holes in gut wall) this can cause food intolerances.
Most common by far is gluten.
Dairy is second most common.
A trial of strictly gluten free diet is always worth doing
Only 5% of Hashimoto’s patients test positive for coeliac but a further 81% of Hashimoto’s patients who try gluten free diet find noticeable or significant improvement or find it’s essential
A strictly gluten free diet helps or is essential due to gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and may slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first as per NICE Guidelines
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
Similarly few months later consider trying dairy free too.
Approx 50-60% find dairy free beneficial
With loads of vegan dairy alternatives these days it’s not as difficult as in the past
Following advice here I have been taking supplements: B12 drops, D3 +K2 drops, igennus Super B-Complex (just 1 tablet) and Magnesium Glycinate. The results to date are below and if I understand things correctly I should now finish with the B12 drops and just rely on the B12 in the igennus Super B-Complex. Not sure why the serum folate level has decreased since taking the Super B-Complex?
In week before blood test, when you stopped vitamin B complex, did you take a separate folate supplement (eg Jarrow methyl folate 400mcg)
Folate level drops rapidly
If didn’t do this ….do so next time
Igennus B complex -Most people only find they need one per day. But a few people find it’s not high enough dose and may need 2 per day and/or may need separate methyl folate couple times a week
SlowDragon thank you. No, I did not take separate folate. Advice noted on methyl folate. I'll keep my eye on it. I have only been taking one Super B-Complex tablet as I was alarmed by the fluorescent green urine on two!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.