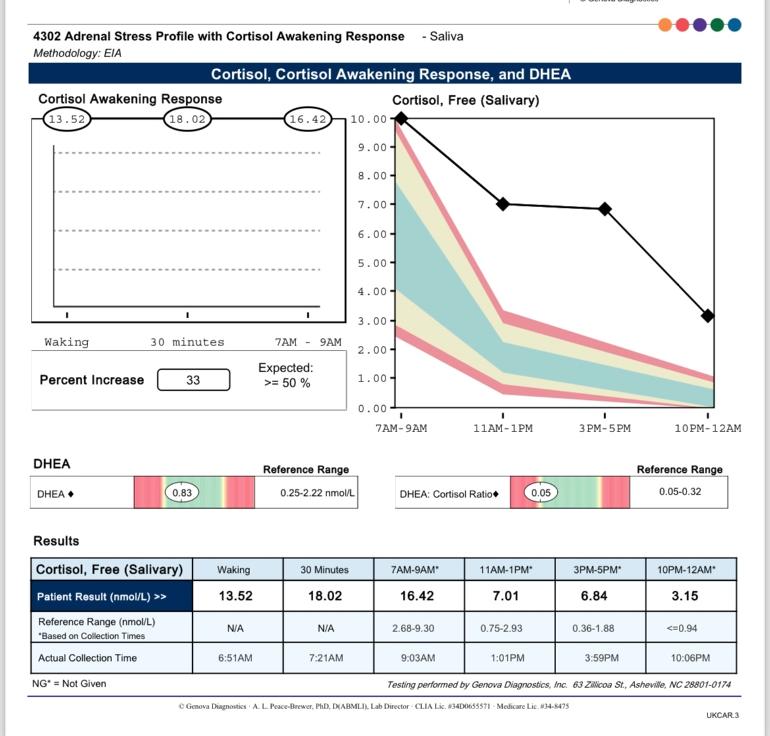
My recent saliva cortisol/DHEA results have returned - Smart Nutrition/Geneva labs came back after 10 working days. I have elevated cortisol and a blunted CAR.
I’m not really sure what that all means but my theory of having low cortisol has gone out of the window! All of my symptoms (except slightly raised BP) match down to salt cravings, postural hypotension, muscle weakness/cramps, intense fatigue (I’m housebound/off work), increased urination, thirst.
I am newly diagnosed hypothyroid and suspect I have been undiagnosed for several years. Central hypothyroidism has been suggested by a v helpful member on here. I am waiting to see an Endo in March to rule out pituitary problems (high prolactin). Am I right in understanding hypothyroidism drives up cortisol? Will continuing on Levo help to bring it down?
I was offered Armour initially but turned it down due to cost. But maybe (due to T3) i might be better suited to it further along and have to suck up the price?
Would taking supplements to bring down cortisol be a good idea? (Ashwanghada, Holy basil, Phosphatidylserine etc?)
I have no symptoms of high cortisol except possibly some slight extra fat around my abdomen in the last few months and difficulty staying asleep after 4am. I am (was until 2 months ago) a masters athlete, so slim and muscular. I don’t have any Cushings symptoms. I don’t drink alcohol or caffeine, eat well, I’ve been pretty much in bed for the last 2 months so not pushing myself at all. I do all the ‘calming’ activities, reading, hot salt baths, extended breathing, my bedtime routine is very strict and always has been.
Are the saliva results useful to see the full cortisol picture? Would blood and urine be helpful to get a fuller picture (tissue vs free vs excreted?). I read a story on here recently of a lady with high saliva, but low blood cortisol. I’d be interested to see, but was also told the Medichecks cortisol blood test is a waste of time due to crap ref ranges. Is there another private blood cortisol test that is more reliable?
I’m on HRT and read this can sometimes give high cortisol results, but I’m reluctant to stop this abruptly for any re-testing.
It’s annoying as I have really high histamine spikes which I had linked to low cortisol so not sure if that’s the case anymore (cortisol being anti-inflammatory). Maybe that’s an oestrogen fluctuation issue, gosh this is all so complicated!
Other noteworthy observations; my body crashed out after two back-to-back v high stress events. This lead me down the adrenal insufficiency/fatigue pathway….but not sure you can have high cortisol with adrenal insufficiency?
What should I do next? Start some adaptogens that regulate cortisol? Wait and get a blood cortisol test to see if that’s low or high? Do nothing and wait to see what Endo says in March. I’m due an increase in levo from 50mcg to 75mcg in January (private thyroid dr).
Written by
GussyG
To view profiles and participate in discussions please or .
Suggest you hold on and get Levo dose slowly increased upwards over several months and then retest
Cortisol levels should settle once thyroid levels are optimal
50mcg levothyroxine is only standard starter dose
Even if we frequently start on only 50mcg, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or somewhere near full replacement dose (typically 1.6mcg levothyroxine per kilo of your weight per day)
Adults usually start with a dose between 50 micrograms and 100 micrograms taken once a day. This may be increased gradually over a few weeks to between 100 micrograms and 200 micrograms taken once a day.
Some people need a bit less than guidelines, some a bit more
TSH should be under 2 as an absolute maximum when on levothyroxine
If symptoms of hypothyroidism persist despite normalisation of TSH, the dose of levothyroxine can be titrated further to place the TSH in the lower part of the reference range or even slightly below (i.e., TSH: 0.1–2.0 mU/L), but avoiding TSH < 0.1 mU/L. Use of alternate day dosing of different levothyroxine strengths may be needed to achieve this (e.g., 100 mcg for 4 days; 125 mcg for 3 days weekly).
Thank you SlowDragon. I’m looking forward to my dose increase as I don’t feel like the 50mcg is doing anything so far. I’m 75kg and tall 5ft8 so on 1.6mcg of body weight that would be 120mcg so around end of April/June to be on 125mcg if going up in 25mcg increments.
When one’s thyroid fails over time (which is our slow burn “engine” for energy), then the body switches over to our turbo boosters (ie, adrenal system and cortisol.)
Early treatment for thyroid starts a slow process of your body correcting it all back. All our hormones are connected - hypothalamic, pituitary, adrenals, sex hormones. It’s all a big chain reaction especially when one malfunctions.
I haven’t read your past posts/profile but depending on how long your thyroid issues were undiagnosed - you might want to set your expectations for 6-12 months on thyroid hormone replacement before tinkering with the other things.
The rule anyway is - change one thing at a time, go low and go slow. Give your body time to Let this first change settle.
Thank you FallingInReverse, wise words of patience. I’m not sure how long I’ve been hypo, it was discovered by chance when I started HRT some two years ago. I suspect thinking about it it’s been much longer, but you get used to feeling cold and knackered all the time!
Quite different to what you were expecting, glad the results came through pretty quickly.
It's not too surprising having only just started on Levo your body has built up high levels of cortisol as thyroid hormones are needed to metabolise and clear the excess so hopefully as you increase your dose things will start to even out
Still not great for coping with MIL though 😬good luck with that 🤗
Ha thanks TiggerMe, it’s reassuring to hear that the thyroid may be the culprit with the cortisol, I’ve been going down all sorts of rabbit holes trying to figure out the causes as it was so sudden and directly after my competitions. Maybe training for 5 years with a wonky thyroid and my body just said, nope, no more!
I’ve managed to negotiate one day at the MILs lair. Just need to get through that 😂
Yep, sounds like you built up to a level your body just can't deal with 🫤
I'd suggest nipping out to get some CBD oil which might make MIL a little more bearable but I also found it lowers cortisol (not something I needed but it monged me out 🤣!)
Perhaps try some of those TRIP drinks as alcohol wouldn't be wise 🙃
Your theory of having low cortisol remains balanced on the ledge of the open window. As you are on HRT (I don't know which type) the results of any cortisol testing may be falsely elevated.
The relationship between thyroid and cortisol levels in humans is something still being debated (and hopefully researched, although I don't know of any studies happening right now).
The Pituitary Foundation is probably the best place to ask about your high prolactin level.
The Pituitary Foundation and the Addison's Disease Self Help Group (which does adrenal insufficiency generally, not just Addison's) are good places to ask about adrenals, cortisol etc.
If there is the possibility that you have adrenal/cortisol problems, do NOT take NDT. The warning information for NP Thyroid® (one form of NDT, but this will be true of others too) says that it "is contraindicated in patients with uncorrected adrenal insufficiency" (ref. npthyroid.com/ )
Taking supplements to try to affect cortisol levels is, IMHO, a terrible idea. The body is very sensitive to changes in cortisol levels, and using unregulated supplements that do not quantify how much of any active ingredient is present, nor guarantee the same level from batch to batch, is not a good idea.
Saliva results are considered useful for checking high cortisol levels if there are no other factors involved. However, whilst on HRT or taking supplements such as the ones that you mentioned, I would not personally consider them useful.
Yes, high cortisol and adrenal insufficiency can be related in certain situations. One example is a cyclic-ACTH producing cyst, that makes ACTH go up and down, and hence cortisol go up and down.
My opinion - set yourself up for a reliable set of blood tests. Settle your levothyroxine dose for at least 6 weeks, stop HRT for 6 weeks, avoid steroids on the morning before the test and ideally the afternoon/evening of the day before as well if safe to do so. Wherever possible, only change one thing at a time, so that if you do get new symptoms you have a fighting chance of identifying why. Then, have an early morning (8-9am) cortisol blood test done. Once you have the results of that, there'll be some useful evidence to work with. If that level is low or high, contact the endo prior to your appointment so that he/she can arrange other tests as appropriate before your appointment. That way, the appointment can be useful rather than being nothing more than the endo filling in blood test forms (this is assuming that the endo knows about cortisol-related issues, something that cannot be assumed).
BTW, contrary to an answer to one of your previous posts, the reference range on MediChecks blood cortisol is clearly shown as 133 - 537nmol/L. Whereas you normally just get notified when the website is updated with test results, with cortisol levels well outside the norm, they get hold of you directly - it is probably not an exaggeration to say that MediChecks cortisol testing may well have saved my life this time last year - they got onto me to tell me to see a doctor within 6 hours when they saw my result! That's how serious cortisol-related issues are, and why I would strongly suggest ignoring anybody who suggests using adrenal cortex etc - if you have cortisol-related issues, find a qualified doctor who uses regulated medications.
I suspect the comment would have been about Medichecks saliva cortisol test with a range starting from 0 ( so rather ridiculous) rather than serum
I've done several cortisol saliva tests and non of them require stopping HRT if transdermal, I don't understand what could be gained from results which would have skewed hormone levels and made someone feel utterly awful in the process?
TiggerMe The incorrect answer to a previous post was in answer to a question explicitly about blood tests, not saliva tests.
As I said in my answer to GussyG , we don't know the nature of the HRT that GussyG is using. Whilst it is accepted that transdermal HRT has less effect in terms of falsely elevating cortisol results, that does not mean that the effect is zero, and anecdotally there are people with diagnosed adrenal insufficiency who have reported significantly elevated cortisol results from transdermal HRT. I cannot vouch for the reliability of those reports, but they are from people who have repeatedly demonstrated good knowledge and experience of adrenal insufficiency, diagnosis and management.
"is it worth doing a quick Medichecks blood cortisol to get an idea of what I’m dealing with ie high or low cortisol?
Personally I think it would be a waste of money. Some of the reference ranges provided are of the form (using made up numbers not real ones) :
Result < 3.6 Range < 2.4
How can one interpret such a stupid result and range?"
So it suggest Medichecks use a greater than rather than actually giving a range which as the above comment suggests isn't a range and isn't useful... can't argue with that 🤷♀️
Perhaps there was some confusion as to saliva or cortisol but I personally don't use Medichecks these days
I'm not suggesting HRT would have no affect on cortisol levels but I can't see what use the results would be if your body requires HRT to function and is your normal state🤷♀️
TiggerMe That's the comment and it's factually incorrect as MediChecks does give a range (see my earlier response), so one can argue with that post.
Ok, yes, I agree that requiring artificial conditions rather than normal state conditions for testing can seem illogical, and in some cases (such as staying off asthma inhalers before cortisol testing) can be downright dangerous. However, there are various reasons for doing it this way. Probably number 1 on the list is that by getting all patients to the same state for testing, there only needs to be one way of interpreting results (i.e. there is one data set that interpretations are based on). The alternative would be that there would have to be a data set for each formulation and dose of HRT, and even then the results would be dependent upon the user using the HRT in the same way at the same time offset to testing. That's a lot of possible data sets and variation in reliability. Get all the patients to stop HRT and there's only one data set and no variation based on usage.
Mistakes get made so worth taking up with the original poster to correct for future readers of the thread, no one likes to leave misleading responses
HRT is just used to bring hormones to a symptom free level and hold them steady, I can't think how the test is any use for women pre-menopause who's sex hormones are fluctuating wildly so absolutely no chance of getting comparable results from one test to the next?
This is the marvellous thing about being in control of sex hormones, no fluctuations 😅
I personally cannot see the point of a result based on anything other than my daily norm 🤷♀️ might as well test someone else! For their research they might like us all on a level but the results are worthless and useless
I've found the saliva cortisol tests very useful as they give free levels and DHEA, less so the blood serum total cortisol and DHEA-S
I have to agree that stopping HRT would cause a big change to my system. I’d probably start having hot flushes and my histamine may flair up. It currently flairs up during my cycle on HRT when I ovulate and before my period, when oestrogen rises and drops - previously it didn’t, but since I’ve been in this current low energy ‘state’ following the high stress events it’s highly unstable. Also we’re talking about changing my system after a 2 year periodisation. If I was to stop it would have to be a very gentle taper over weeks/months and watch for symptoms mentioned above.
JumpJiving what is the reason for NDT contraindicated with uncorrected adrenal insufficiency? Presumably it’s to do with the T3 part as Levo is ok?
GussyG I didn't know the answer to your question so I Googled it. Google popped up a document on the FDA website that says the same about Levothyroxine. What it says is:
"Levothyroxine is contraindicated in patients with uncorrected adrenal insufficiency since thyroid hormones may precipitate an acute adrenal crisis by increasing the metabolic clearance of glucocorticoids"
That seems to say that if both hypothyroid and AI are suspected, get the AI under control and stabilised, then sort the thyroid but being prepared to increase the HC dose for AI when adding thyroid hormones.
For me, I was already on levothyroxine long before developing AI, but I found that when I started on HC that I also had to increase my dose of levo and then nudge up the HC very slightly before stabilising, so seems to tie up.
and GussyG from what i understand (which is 'little') the issue is with any type of thyroid hormone replacement, it definitely does include levo .
If AI is present but untreated ,then adding thyroid hormone can cause adrenal crisis . so the AI needs to be diagnosed and corrected first.
i don't know if high cortisol can be present with AI , so i don't know if adrenal crisis is a risk in this case or not ... interesting about that cyclic acth cyst you mention JumpJiving.
but given there is clearly something significantly wrong with the cortisol levels here , if it was me , i would want an endo to do a bunch of tests to get that issue properly diagnosed without muddying the waters by taking anything to try and alter cortisol before they had chance to do further testing .
and i'd make sure whoever prescribed the thyroid hormones is made aware of these high cortisol results.
I am quite worried that I have some kind of adrenal insufficiency, many of my symptoms match (although they also cross over with some hypo symptoms- like muscle cramps and fatigue) but I had a severe dizzy episode recently where I got up at 5am to use the loo and was completely’drunk’ in my head and couldn’t walk. I had to lie in the floor and call my partner, it was scary. Not like passing out either. I’ve NEVER experienced this before in my life. I also have black gums, thirsty, postural hypotension.
What if adding levo for the last few weeks has actually caused my cortisol to rise up? I’m genuinely quite concerned now. The GP is useless. Told me fibromyalgia or anxiety.
p.s i think ? the issue is that adding thyroid hormone can make the body use up cortisol faster ... so if it's already too low , then adding thyroid hormone without dealing with that first could cause cortisol to drop through the floor, causing adrenal crisis ( which is a big problem . and i assume potentially fatal)
but remember . i know nothing about this other than the very basic warnings i have read in medicine leaflets .
GussyG I don't think you had mentioned the black gums before. Darkened gums can happen as a result of hyperpigmentation resulting from high ACTH. The most common cause of high ACTH is primary adrenal insufficiency (Addison's), but as your cortisol appears to be high (sometimes at least) it would be worth investigating the possibility of the cyclic ACTH-producing cyst. Both require a referral to an endo, but the latter requires a referral to a good endo. It's not a guarantee of quality, but you might want to start with a Pituitary Centre of Excellence when getting the referral.
There are, of course, other things that can cause dark gums, but those would also want a doctor to look at, so please follow up with a professional medic sooner rather than later.
When you do see an endo, make sure to have a list with you of every symptom that you have, no matter how odd they might sound. Some of them may be very specific to certain conditions, others might give a clue that when grouped with others also suggest a certain condition. I had a long list of symptoms caused by tertiary adrenal insufficiency that wouldn't have meant anything to my GP or even an average endo, but should have done to a really good endo.
Ok thank you tattybogle and JumpJiving I think that’s all my brain can handle for today. I’ll have to come back and re-read again tomorrow! All I know is I have to wait until March to see the Endo (this was an urgent referral) to my local hospital. I’ve got their name but no idea if they’re good or not. How would I go about getting a referral using Pituitary Centre of Excellence?
I do hope the continuation of levo doesn’t add anymore fuel to the fire if adrenals are involved. What to look out for other than collapsing in a heap? JumpJiving you mentioned you were on Levo before being treated for AI. Can you tell me more about your symptom progression and how it got picked up? (If you don’t mind?)
Ask your GP to refer you to an endo at one of those (do some research first to check on what patients think of the endo's). I only hear recommendations for one particular endo at my nearest Pituitary Centre of Excellence.
The things to be aware of are symptoms of pending adrenal crisis. Adrenal crisis can come on very quickly, so act quickly if you think that is what is happening. Symptoms of adrenal crisis can be found at pituitary.org.uk/app/upload...
Unfortunately, my symptom progression is likely to be different as mine is tertiary AI (and I had one symptom that is so rare that I doubt I'll ever meet an endo who has heard of it). With tertiary, it's not uncommon to have high blood pressure, whereas with primary it's typical to have low blood pressure. Sometimes, symptoms get really confused - for instance, I had serious salt cravings (and foot cramps), which is typical of primary, and not expected in tertiary. I also had postural hypertension, again common in primary, not normally expected in tertiary. So, it can get a bit weird - even within the same diagnosis, the progression varies. Increasing fatigue and dizziness, and weight change (weight loss when cortisol low, weight increase when cortisol high) are common though.
It might have been me who wrote that comment about Medichecks ranges. I remember reading about their ranges for saliva cortisol testing and they were as I described. But it was quite a long time ago and they may have improved them since I read them.
I really appreciate your informative reply thank you. Also thanks for clarifying the cortisol blood test range.
HRT: I’m on bioidentical Sandrena gel 1mg day and continuous Utrogestan (1 at night). It very much affects my system and I’m not a believer (certainly for me) that topical is any less potent than oral. I’m sensitive to it. In fact I have wondered if the oestrogen component has exacerbated my (back then undiagnosed) thyroid symptoms. I was put on it originally for poor sleep and hair loss, brain fog and being 46 and in peri (shorter cycles). But I now know these symptoms are also classical thyroid symptoms. My body has built up a tolerance to it now and I’d be nervous to stop it. Having said that I’m also keen to rule in or out any other issues. I’ve been close to taking myself to hospital twice the last few months feeling so bad.
I don’t take any steroids and I’m not taking any supplements to lower cortisol, I just take a usual suite of vitamins for optimal thyroid function. I was just thinking out loud to see if anyone had any thoughts on trying to lower cortisol. But understand what you’re saying and don’t want to muddy the waters. I’ll keep it simple and allow more time before a blood test.
I’m an unusual and a frankly weird case but I found thyroid meds send my histamine levels off the charts and this in turn greatly impacts my cortisol levels.
So when my histamine levels are high, my cortisol is completely off the charts high (apparently histamine is inflammatory and cortisol is an anti inflammatory so it would make sense that cortisol is high and trying to get control of the inflaming histamine!)
My prolactin climbs higher the more thyroid meds I take…does this happen with you?
Interesting, so I’ve not noticed any increase since I started my thyroid meds, which led me to conclude mine were/are triggered by stress (I had two clear very high stress events) with high cortisol, but also I had further problems with my body reacting in that stressful time when my hormones dropped before my period and rose and dropped during ovulation. So I had less resilience to the hormonal fluctuations if that makes sense? It’s all linked somehow. I also read somewhere about the link with all of this and oestrogen dominance…
Have you retested your cortisol recently? I’d like to do mine again but can’t afford it.
I’m due to have my prolactin retested this week after x2 over the range readings and the NHS lab ‘losing’ my latest result 🙄. I’ll have been on thyroid meds for 3 months so it will be interesting to see if it’s come down or gone up. (I still feel like crap!)
I have to say I’m a little jealous…when I started levo my reactions were immediate and vile (although at the time I didn’t realise it was histamine!)
I haven’t retested cortisol for awhile but gonna redo a saliva cortisol soon I think.
I’m also going to request a Synacthen from my endo (it’s hard for me to stop the contraceptive pill so I’d need to book 6 weeks off work to do it and won’t be able to even consider that until the summer really)
Interested to hear about your next prolactin levels! I think technically levo is supposed to help it normalise but this was absolutely not the case for and it eventually got so high it was affecting my dopamine levels and making them undetectable!
You should ask them to do a canulated prolactin test too if it’s still raised!!
Would taking supplements to bring down cortisol be a good idea? (Ashwanghada, Holy basil, Phosphatidylserine etc?)
I found out that I had high cortisol from saliva testing a long time ago. Three out of four saliva samples were over the range. The single sample which was in range was about 90% through the range. Much more recently I had a blood test for cortisol at 8.30am - 9am and that was over the range too.
I struggled to tolerate thyroid hormones when I first went on them (in 2013) but found that if I took my first thyroid hormones of the day when my cortisol was closest to optimal for the time of day I could tolerate them.
When I was researching high cortisol I found out about Ashwaghanda, Holy Basil, Phosphatidylserine, and Seriphos. My results for all of these were :
Ashwaghanda - made me nauseous so I couldn't take it
Phosphatidylserine (PS) - couldn't afford it
Seriphos aka Phosphorylated Serine - I think this might have actually been working to reduce my cortisol but it made me feel like I had severe flu and I couldn't tolerate it for more than a month
When I was experimenting with the above the PS was more expensive than Seriphos. But at some point the reverse became true and the Seriphos became more expensive than the PS. I don't know the current situation.
Holy Basil was by far the cheapest thing I tried and was the one I took long term. I stayed on it for nine years. It helped me with my lifelong insomnia as long as I continued to take it. I always took it at bedtime. But then, for unknown reasons, I developed a severe intolerance to it and had to stop taking it. It was giving me the indigestion from hell rather than allergy symptoms.
The blood test I mentioned further up was done just before I stopped taking the Holy Basil.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.