I posted earlier today and members have been really helpful. I am going to call my GP surgery tomorrow as you have advised and request my results electronically/paper since my diagnosis. Below is the information I have been given over the last 12 months (verbally)
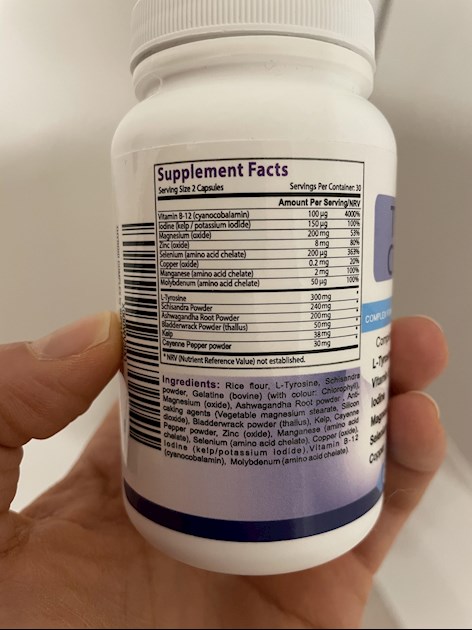
I have been on 75 mg levothyroxine since October 2021. I take over-the-counter vitamin D (3000 IU) and supplements to support thyroid (see photo).
I am new to this and have begun to feel unwell again since January. I posted on here today about how do I access a specialist. Members today have advised me to get blood tests first before seeking private specialist. GP will not refer me and did not want to retest for another 12 months. (He then changed this to retest in 6 months )
TSH range: 0.3 - 4.2 Vitamin D (told over 50 is normal?)
Verbal Results:
Feb 2021 - TSH 44 (Extremely high) Vitamin D (told below 12)
May - TSH 10.01 Vitamin D (told normal)
Sep 2021 - TSH 5.6
Dec 2021 - TSH 2.3
Feb 2022 - TSH 4.49
Any guidance and advice most welcome
Written by
Browneyes100
To view profiles and participate in discussions please or .
That is a terrible supplement. And, I'll tell you why...
B12 - cyanocobalamin: The cheapest, and least bio-available form of B12. You'd be much better off with sublingual methylcobalamin. But, no point in taking just one B vit, because they all work together and need to be kept balanced. So, you'd need to take the methylcobalamin plus a B complex.
BUT, before taking any B vits at all, you should have your B12 and folate tested, to see IF they are low, and HOW LOW they are. A B12 blow a certain level should be investigated by testing for Pernicious Anemia. But, now, as you've been taking B12, you'll have to wait a few months to get a base-line.
Iodine/kelp: About the worst thing you could take for your thyroid unless you are deficient. And, even then, there are protocols to put in place first, and the treatment needs to be supervised by an experienced medical professional.
Iodine in excess can cause all sorts of problems, and is also anti-thyroid - used to be used to treat Grave's before anti-thyroid drugs were invented. And, as you're already taking 75 mcg levo, you'll be getting about 50 mcg iodine from that, which is recycled in your body, plus what you get from your food, and you're probably well over the recommended daily intake.
Magnesium oxide: the cheapest and least bio-available form of magnesium.
Zinc and copper: these two need to be kept balanced, but hypos are usually high in one and low in the other - very often low in zinc, high in copper - so taking more copper is a very bad idea. Both should be tested before supplementing.
Ashwagandha: can lower cortisol. So, if your cortisol is already low, as it often is with hypos, lowering it even further is not a good idea.
Mult-vits are never a good idea, for all sorts of reasons. Best avoided.
Please don't take any supplements with iodine or kelp - these can be really unhelpful.
And multi-vitamins generally aren't recommended here - they tend to include thing you don't want or need, so it's usually best to test key nutrients - ferritin, folate, vit D and B12 and just supplement individually what you need to.
Tagging SeasideSusie SlowDragon and greygoose to add more
And your thyroid results are (a) not great and (b) inadequate so it's no surprise you don't feel great
Once on levo, you need regular increases (25 mcg a day at a time) until TSH is ALWAYS less than 2 and probably less than 1 - and your thyroid hormone are nice and high in range. Which means testing free T4 (which is pretty basic) and free T3 (which is often harder to get the GP or the lab to do) although this is the most important result, as it shows the amount of active thyroid hormone available for your body to use - and this needs to be good (at least 2/3 through range) for you to feel well.
So please go back to the GP and ask for a dose increase (as per NICE guidelines) as TSH is still much too high (and indeed over-range) - and for him/her to do the other tests you need. Remember to have an early morning (before 9am) fasting blood test and leave 24 hours from your last dose of levo
Thank you. This is why I am frustrated. I asked for an increase and a referral. He said ‘no’ because it’s ‘just above normal’. I tried to challenge. I feel not listened to and trying to navigate this elsewhere
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
NHS England Liothyronine guidelines July 2019 clearly state on page 13 that TSH should be between 0.4-1.5 when OPTIMALLY treated with just Levothyroxine
Note that it says test should be in morning BEFORE taking levothyroxine
As I have been taking the supplement in the photo, should I wait a period of time without taking the supplements before going for tests? If so, how long for?
Excuse me for jumping on this Post , why Monday & Tuesday as I have been trying for a 9am test from Medichecks and have managed to get one on Wednesday this week ? .
First thing I would say is to stop the thyroid support supplement, it could make things worse.
It contains iodine and we shouldn't take that unless tested and found to be deficient. The recommended daily amount of iodine is 150mcg and in the UK we can easily get that from a normal diet containing milk and other dair products plus white fish such as cod and haddock. That supplements contains that amount plus 38mg kelp which contains iodine as well. Iodine solution used to be used to treat hypERthyroidism before the current radioactive iodine treatment, and it can make hypOthyroidism worse.
It also contains Ashwagandha which is know to lower cortisol and again you would need to know your cortisol level before taking anything that can mess with it.
The B12 it contains is the cyanocobalamin form which is not recommended, the recommended for is methylcobalamin.
It contains magnesium oxide which is poorly absorbed and usually used as a laxative.
It contains zinc oxide, again a form not recommended (it's found in nappy rash and sun creams) and we shouldn't take zinc unless we know we need it. Zinc and copper should be balanced and we hypos tend to have one high and the other low, so we need to know those levels before we supplement. Zinc reduces the amount of copper the body absorbs, and high doses of zinc can cause copper deficiency.
What you should do is get the key nutrients tested as mentioned earlier and see where your levels lie then if necessary supplement accordingly.
Vitamin D (told below 12)
Seriously? Your Vit D level was below 12nmol/L? That is severe deficiency and were you given loading doses of D3?
I take over-the-counter vitamin D (3000 IU)
You really need an up to date test to see if you are taking the right amount of D3. We should test twice a year when supplementing.
Also, when taking D3 there are important cofactors needed - magnesium and Vit K2-MK7. Are you also taking these?
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc. 90-100mcg K2-MK7 is enough for up to 10,000iu D3.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 I like Vitabay or Vegavero brands which contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
If looking for a combined D3/K2 supplement, this one has 3,000iu D3 and 50mcg K2-MK7. The company has told me the K2-MK7 is the Trans form
Magnesium helps D3 to work. We need magnesium so that the body utilises D3, it's required to convert Vit D into it's active form, and large doses of D3 can induce depletion of magnesium. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
TSH range: 0.3 - 4.2 Vitamin D (told over 50 is normal?)
Verbal Results:
Feb 2021 - TSH 44 (Extremely high) Vitamin D (told below 12)
May - TSH 10.01 Vitamin D (told normal)
Sep 2021 - TSH 5.6
Dec 2021 - TSH 2.3
Feb 2022 - TSH 4.49
Presumably you were started on Levo after the February 2021 and May results?
How much Levo do you take?
Your February 2022 TSH is over range so did your GP increase your Levo? He should have done. If you haven't had an increase then use the following information to support your request for an increase either with this doctor or you may be better seeing a different one:
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
Also, Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He confirmed, during a talk he gave to The Thyroid Trust, that this applies to Free T3 as well as Total T3 and this is when on Levo only. You can hear this at 1 hour 19 mins to 1 hour 21 minutes in this video of that talk youtu.be/HYhYAVyKzhw
You can obtain a copy of this article from ThyroidUK:
tukadmin@thyroiduk.org
print it and highlight Question 6 to show your GP.
This is really useful information l. I had no idea about the different forms of vitamins/supplements. I forgot to mention that I am vegetarian- don’t know if that makes a difference.
I need to go and get the blood tests to check any deficiencies like you advised. I’m also going to get myself prepared with all this information and go back.
The Levo has been given to me incrementally, 25 at a time. But has not changed since Sep/Oct 2021 (75). He would not increase it for me in Feb 22 as it’s ‘just above’ and wanted to wait 1 year! Even though I’m saying that I don’t feel great!
I forgot to mention that I am vegetarian- don’t know if that makes a difference.
Vit D comes from sunshine. Also oily fish, also egg yolk when it's a true free range chicken or chicken is fed Vit D enriched food if you do eat these. I used to be a demi-veggie, ie no red meat but I would eat fish and chicken.
You may be low in B vits and ferritin as a vegetarian.
you are 44 yrs old, and your initial TSH was 44 ...and they started you on just 25mcg ?
Do you have a) a heart condition ? or b) are you the weight of a mouse ? ~ (see NHS guidelines below)
Most of us don't think it's such a great idea to start people on the "full expected dose for their weight" ( even though NHS guidelines do say it can be done...)
.... but starting someone of well under 65 with no heart condition , on just a measly 25mcg when their TSH was 44 ... is .... ridiculously over cautious... and just prolongs the agony. 50mcg is the more usual starting dose for adults under 65 without heart disease.
And should be increased from there as quickly as is sensible (initially in 25mcg increments)
"Managing primary hypothyroidism1.3.3Offer levothyroxine as first-line treatment for adults, children and young people with primary hypothyroidism ..........
1.3.6Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
1.3.7Consider starting levothyroxine at a dosage of 25 to 50 micrograms per day with titration for adults aged 65 and over and adults with a history of cardiovascular disease. "
If i were you, i'd want an explanation of why they only started you on 25mcg.
And given that your TSH has risen to over range again , i'd write to GP referring them to guideline 1.3.6 and request a 'trial' increase to 100mcg now , not in 6 months time.
Here's another reference to encourage your GP to 'get on with it '.. you need your dose increasing now, not in 6 month time .
They have already had plenty long enough to see the effect of 75mcg.. and your pituitary gland (TSH) has clearly decided 75mcg is not enough .. that is why TSH has gone back up again to over 4 :
"The goal of treatment is to make the patient feel better and this tends to correspond with a TSH in the lower half of the reference range (0.4–2.5 mU/l) .If a patient feels perfectly well with TSH between 2.5 and 5 mU/l there is no need to adjust the dosage"
.....But you don't feel perfectly well, so they should adjust your dose.
Ps. it is NOT not in your head, most of us here have been 'helped' to feel like it is in our head at some point , ... and as for the ?menopause? suggestion... it has all sorts of (un)funny effects on all sorts of things~ but it categorically does NOT make TSH go up to 44... so if they start fobbing you off again with the "well , at your age .... " remind them that you have confirmed primary hypothyroidism and you would like them to deal with the symptoms and blood results indicated by that very obvious problem first , before they go blaming how you feel on 'something else'.
Thank you for the advice. You’re right. I can’t just wait another 6 months and hope for the best because I’ve been told to. The data will definitely help.
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
SeasideSuzie and SlowDragon and the others have provided loads of info- much (if not all) of which was given to me. I am well thanks to this forum. If you read my profile it documents my interactions with GPs and how I got what I needed. It also identifies their shortcomings with regards to data interpretation (blood tests). I’ve couched it in humour in places, to make the read less onerous.
They see it as a professional courtesy to back each other up, until they realise they are leaving their arses bare in doing so (then they bring each other up to speed in private) 😉
Thank you. I’ve just read your bio. I can see the rollercoaster you have been on too. So glad you’re feeling better.
I am overwhelmed by the wealth of information on here and can’t wait when I get to the point where I too will become my own expert. I’m in awe of how knowledgeable everyone is. So glad I made the decision to post.
I know people who suspect they are being mismanaged, yet still can’t bear the thought of becoming their own health advocate and knowing for sure.
If you get a knowledgeable Doc it must be brilliant (yet to happen for me and I have seen a different one every time) sometimes the best you can hope for is a Doc who recognises the limits of his own knowledge. I’ve spoken to two like that. I would like to think they took something away from our chats as I backed up my requests with solid information. Paper references do help as do quoting their own guidelines at them 😂👍
Browneyes- well well done for posting. Thats the biggest step in my opinion. Knowledge is power and will enable you to take charge of your health. You will get lots of great advice in here but have a look at Thyroid UK website. They have a list of books to read. A good one to start with is called Living with your Thyroid by Barry Durrant-Pearfield. By the time you've read that you will know more than most doctors about Hypothyroidism - sad fact!
If I remember right thats his earlier book - he then updated it and changed the title. I cant remember what the difference is between them as its been a longtime since I read it.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
