After having some private tests done (results attached), I thought it would be sensible to at least try to go down the NHS route, despite my mum having disappointing reactions from her GP for the past 15 years.
We asked for a referral to an NHS endocrinologist. The GP was dismissive of the private test results and asked for NHS blood tests to be done, the next availability of which is in June...
When I spoke to him about T3 he said that T3 is only administered in emergency situations and essentially told me to stop researching on the internet, as I was being misled.
Obviously this is complete nonsense and sort of expected. We're planning a private consultation with Prof. Jonathan Wass as soon as we get the letter of referral we asked for.
What exactly was the doctor talking about when he mentioned T3 only being administered in emergencies?
Written by
kendrewaddams
To view profiles and participate in discussions please or .
Not true. He may have seen liothyronine in vials in the BNF, these are for emergency use. Her fT3 is quite low given you have highish fT4 and TSH levels. Theoretically low selenium levels could cause this so it would be worth trying a selenium supplement.
When someone suffers from extremely severe hypothyroidism - which can occur quite suddenly in cases of a hypothyroid person having a severe illness or a serious accident, and can also occur in long term under-treatment or non-treatment - there is a condition which can arise called myxedema coma or myxedema crisis, which is a medical emergency. It is fatal in about 50% of cases.
In myxedema the treatment for many years has been T3 into a vein via a drip in a hospital. But since T3 is so expensive in the UK doctors are often now using T4 (i.e. Levo) in a drip and just hoping for the best. I'm sure it will increase the death rate from the condition, but then, I'm not a doctor so take this with a pinch of salt.
Myxedema = US spelling
Myxoedema = UK spelling
I don't think your mother's results are likely to cause myxedema, but they will make her feel absolutely dreadful, ruin her quality of life, and make her more likely to get other health problems e.g. heart problems, osteoporosis, poor gut health, pain.
Your doctor is wrong though, about T3 only being prescribed in emergency situations. There are quite a few people on this forum who get T3 prescribed on the NHS, but it is very, very difficult to get it because it is so expensive.
Many, many doctors would have the same reaction as your mother's doctor. The issue is not that T3 is dangerous (it isn't) or ineffective at making hypothyroid people feel better (it isn't) - it is purely an economic issue.
A number on this forum - including me - get lio prescribed on the NHS without having been anywhere near a coma!
When - as here - your free T4 is over-range and free T3 is under-range, that's a pretty clear clinical need, I'd have thought - so good luck with the endo
Mine is free on the NHS - as are the people on the link that SlowDragon sent - so check out your CCG.
Lio free on the NHS can only be initiated by an endo (after that the GP usually picks up the prescription and related cost - at the bottom mine refers to the "specialist care" of the named endo) - but not all of them will (a) because of the cost (b) because it has a very short half-life so is difficult to measure and (c) because a surprising number of them genuinely seem to think it doesn't work and the thousands of us that have found it transformative are suffering from some huge joint delusion (!)You can get a list of T3-friendly endos from Dionne at ThyroidUK - tukadmin@thyroiduk.org - but be aware that your GP is not obliged to refer you and they are not obliged to see you. You will need to show that - like the OP - you are a "poor converter
Initial treatment should always be to start on levothyroxine. Standard starter dose of levothyroxine is 50mcg. (Always same brand) Increase dose slowly up to full guideline dose of 1.6mcg levothyroxine per kilo of your weight
Test vitamin D, folate, ferritin and B12 at least annually Frequently necessary to supplement to improve low levels to optimal levels
If cause of your hypothyroidism is autoimmune thyroid disease also called Hashimoto’s, Coeliac blood test done BEFORE considering trial on strictly gluten free diet
About 90% of primary hypothyroidism is autoimmune thyroid disease
It typically takes 6-12 months to work through all these steps
If after all these steps, Ft3 remains low.....referral to endocrinologist for consideration of addition of small doses of T3 prescribed alongside levothyroxine
Getting Dio2 gene test privately before consultation can be helpful too
If NHS endocrinologist says you have clinical need for T3....Initial 3 month trial of T3 must be via hospital pharmacy. Assuming trial goes well, endocrinologist formally requests your GP take over care and cost of prescription. Annual review back with endo.
I get my T3 prescribed on NHS
Hashimoto’s, confirmed severe gluten intolerance, multiple vitamin deficiencies and tested positive for heterozygous Dio2. Took 26 years to get prescribed!
Like you, it took years to get it and now I think Endo reluctantly gives it!)
I do believe that from all previous correspondence with Endo it has been found that I need it!
Next week I am moving to Shropshire and am really worried that when I register with new GP, I wont be allowed my T3 prescription!
I want to be as prepared as I can be!
I am planning on registering with GP putting in a prescription and seeing what happens but that may not be the sensible thing to do! But I am concerned about running out!
A lady on here has kindly given me a recommendation for an Endo in Shropshire but would need a referral from new GP.
If it has been established that you cannot convert by an NHS Endo is that ammunition enough to say you have to have it or is it just a lottery?
Your mother's results are not good, and there are various things she could do to help herself feel better.
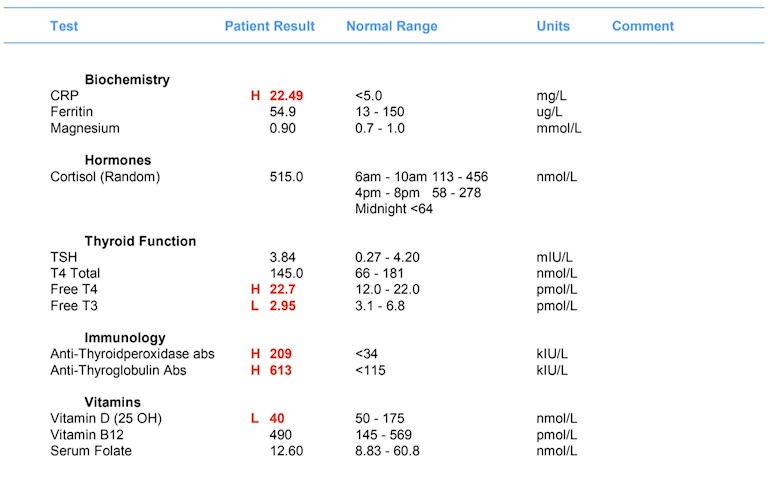
CRP --- This is a measure of inflammation which is very common in people with hypothyroidism. It also becomes high in cases of infection. Unfortunately, CRP doesn't tell people what the problem is, what is causing problems, or where it is. Optimising nutrient levels and thyroid hormones will help to reduce this. Optimal for CRP is < 1.
Ferritin --- This is a measure of your mother's iron stores. Your mother's result looks, superficially, not too bad. But it is under optimal. High CRP can also raise ferritin, making it look better than it really is. Optimal for ferritin is roughly mid-range or a little bit over. It would be a good idea to get an iron panel done, if possible, but delay doing this until other things have started improving, since it doesn't look dramatically bad at the moment. If your mother suffers from restless legs or hair loss this could be because of low iron, and some people need to raise their ferritin to over 80 to improve these.
Magnesium --- This is not a reliable test. About 0.5% of the body's total magnesium is found in the bloodstream. The rest is found in organs, bones, muscles etc. If magnesium levels drop in the blood the body steals it from other tissues. So, blood levels of magnesium almost always stay looking good in blood testing, even if the body is deficient.
The good news is that people with functioning kidneys can supplement magnesium without testing. Excess magnesium is excreted in the urine. Anyone taking magnesium supplements should become familiar with the symptoms of excessive magnesium, just in case it starts to build up. (Nobody has ever mentioned this ever happening on the forum, as far as I know.)
If your mother suffers from muscle spasms, eyelid tics, or cramp then it indicates low magnesium is likely to be a problem.
Cortisol --- This is rather high, and this could be caused by her low nutrients and poor conversion from T4 to T3. When the body is short of thyroid hormones it is normal for the body to produce more cortisol and adrenaline (both of which are stress hormones produced by the adrenal glands) just to keep the body going.
TSH & Thyroid Hormones --- Your mother's TSH is most likely to be higher than optimal because her T3 is low. TSH is affected by levels of both T4 and T3. In people who are hypothyroid TSH is optimal at 1 or under, although everyone has to find their own sweet spot. Your mother's conversion (from T4 to T3) is very poor. Improving nutrient levels will help.
Thyroid Antibodies --- Your mother's results indicate that she suffers from autoimmune hypothyroidism (what UK doctors call it), also known as Hashimoto's Thyroiditis or Hashi's (what patients on this forum call it). But 90% of cases of hypothyroidism in the UK are of this type, so it is very common.
Vitamin D --- Your mum's level is extremely low. She needs to supplement. To work out how much vitamin D is needed, use this calculator :
Supplement with Vitamin D3, NOT Vitamin D2. The best kinds, easily sourced online, are either capsules containing nothing but Vitamin D3 and oil, or mouth sprays.
Vitamin B12 --- In your mother's shoes I would want Vitamin B12 higher than it is. Top of the range is a good start, but the reference ranges in the UK are (allegedly) much lower than they are elsewhere. In Japan the top of the range is allegedly around 1300 ng/L, and they regard anything under 500 to be deficient. Vitamin B12 is the only nutrient I would be happy having over the range. A good supplement for B12 is methylcobalamin. For future reference the Active B12 test is a better test than serum B12, but optimal is different.
Folate --- Optimal is the upper half of the range i.e. about 35 - 60 with the range from your mother's results. A good supplement for folate is methyfolate.
Summary& Suggestions --- CRP and Cortisol may improve themselves with optimised nutrients - they can't be improved directly. Instead we have to improve other things in the hope of reducing symptoms, CRP and Cortisol.
I would suggest that your mother needs to start taking some supplements as a first step, but only add them one at a time with about a week between each addition.
The first one to be supplemented should be vitamin D since her level is low.
Vitamin D Supplements increase absorption of calcium from the diet. That calcium needs to go into bones and teeth, not end up lining the arteries. To achieve that we need to supplement Vitamin K2 and Magnesium. Look through SeasideSusie 's replies to others to see what she has to say about vitamin D, magnesium and vitamin K2 :
Since your mother's B12 and folate aren't outrageously bad she may do well with just a Vitamin B Complex. The two most often mentioned on here are :
Thorne Research Basic B - Full dose is one a day.
Igennus Super B - Full dose is two a day.
I would suggest taking full dose for, say, three or four months. Then switch to Igennus (if taking the Thorne) and take one a day. Some people feel better on the Thorne though. It's trial and error.
Going Gluten-Free --- This is very important and should be tried by anyone with hypothyroidism, for three months (and probably for ever if they get benefits from trying it). Going gluten-free has a huge impact on symptoms in those who do get a benefit. But people can't be "almost gluten-free". It has to be 100% or nothing. There are some people who get no benefit from this experiment, in which case after a three month trial they can go back to eating gluten again. Going gluten-free may reduce thyroid antibodies in some people - although antibody levels fluctuate anyway. Whether this helps to feel better or not seems to depend on the person. If going gluten-free works to improve symptoms it may reduce CRP.
Adding T3 to your mother's thyroid treatment --- Ultimately, this may be the only option your mother has to make a big impact on her health. Since doctors will hardly ever prescribe T3 many of us have to buy it online. It can be nerve-wracking. If you decide to try this then write a post asking for sources of T3 to be sent to you via private message (we can't discuss sources publicly on the forum - it is against forum rules). If you check out any sources you get sent and decide which you want to try, send a private message to one of the Admins and ask if they have any information or feedback on the source you've been given i.e. do they know anything to suggest you may have picked a scammer. Note that some scammers are members on here and they answer these requests for sources, so we have to be wary.
Ferritin --- I haven't mentioned this in any detail. If the suggestions I've made help then your mother's CRP may fall. This may then lead to Ferritin dropping too. This isn't bad - it just means that the result is more believable because it isn't being affected by inflammation.
If you're interested, ferritin and inflammation are related by ferritin being an acute-phase protein - but you don't need to know this :
Amazingly helpful thank you! This was really comprehensive and extremely useful. I started her on a 3000ui vit D spray with K2 yesterday and have a B complex ready to go in a few weeks.
I'll definitely be coming back to this post for reference!
We should hopefully have a consultation with the private endo in the next couple of weeks and so will see where we can go with T3 from there.
That has to be one of the best replies I have ever seen on here Human Bean. I had a quick look at your profile and all I can say is in reply to your "I'm not a doctor nor do I have any medical training" is, you could have surprised me! If only our GPs could be half as knowledgeable as you
I'm a thyroid and related subjects gal with a strict emphasis on the practical. When it comes to the nitty-gritty and the biochemistry I would leave that to helvella. If anyone ever asks about the care and feeding of heart attacks or cirrhosis of the liver or broken legs or kidney failure I'm not volunteering anything on those.
FMESG reviewed an updated final draft of the RMOC Guidance for Prescribing of Liothyronine. Key changes in the updated guidance included clarifying the roles of GPs versus NHS consultants in the withdrawal or adjustment of liothyronine treatment, additional guidance to strengthen the need for endocrinology involvement for use within psychiatric indications, and amended wording of ‘no benefit’ to ‘lack of evidence of benefit’.
Helpful comments had been gathered from endocrinology; these were in support of the recommendations from RMOC, however emphasised that the recommendations around use in treatment resistant depression could be made stronger to prevent initiation in the first place.
The group considered that the current GM position is largely in aligned with the RMOC recommendations; with the exception that liothyronine is GREEN (following specialist initiation) where RMOC recommends that share care arrangements should be considered.
It was noted that RMOC provided a helpful example template for shared care and that adoption of a similar protocol across GM may help ensure that any new initiations are done in line with GMMMG recommendations.
FMESG agreed to amend the current positioning to AMBER and retain the current GREY listing criteria, but remove the recommendation for annual review by an NHS (4) endocrinologist as it was agreed GP review was sufficient. Instead provision should be made within the SCP for GPs to refer back to endocrinology if TSH level is abnormal (in line with RMOC example SCP).
ACTION: FMESG recommend liothyronine (T3) be AMBER and GREY; where levothyroxine has failed, endocrinologists treating patients under the NHS may recommend liothyronine in exceptional circumstances for individual patients after a carefully audited trial of at least 3 months duration, in line with BTA guidance. This recommendation to be opened for GM-wide consultation and pre- support to action sought from October CSB. RDTC to identify author for SCP.
You are correct. She should be referred to an endocrinologist as they can prescribe T3 if her T3 is low, not just if she's in a coma. This is in accordance with NICE guidelines. I would write a letter of complaint to her practice complaints manager, also include a print out of the relevent nice guidelines, it isn't right that doctors can make excuses up as a reason to prevent proper treatment. I am going through something similar for a different health condition.
As others have said your Mum really needs some T3 added in and levothyroxine reduced as shes clearly a poor converter. You can get T3 on the NHS via an endocrinologist if they say you need it. I have ndt on the nhs, prescribed and under written by a nhs endocrinologist. The NHS has made this a more ardous process because of cost principally. It isnt a quick process but if you can get it this way it will save a lot of money. It terrible that people end up buying their own when we have a nhs we are paying for out of income! I too had to buy my oen ndt for several years prior to the nhs prescribing.
Human bean has given some excellant advice.
Optimising minerals and vitamins is very important and commonly low in hypothyroidism.
A vitamin D level of 40 is low -symptoms of vit D deficiency are non restorative sleep, aches and pains and constant fatigue, low resistance to viruses and taking longer to recover from them. Your GP may not prescribe the vit D at this level but it is worth asking for a course. She needs level to be over 80, preferably around the 100. You do not excrete excess vit D so follow up vit D blood test after three months is important. It is wise to have your vit D checked annually. Vit D is needed for the absorption of calcium. With low vit D your body will excrete calcium from your bones to compensate for what it cant absorb from food and ultimately this can lead to bone weakness causing fractures. I know this happened to me -my vit D level was very low at6 but am ok now since treatment.
Hi kendrewaddamsI'm fairly new to thyroid conditions after being diagnosed with hyper in 2018 then in 2019 having my thyroid removed I became hypo.. But what I want to share with you is the utter contempt of some GPS and endos in diagnosing these thyroid conditions, it took my gp and endo 2 years to eventually agree I had hyperthyroidism, only when I went in to thyroid crisis and was admitted to hospital in a near coma did my gp and endo sit up and take notice, to late I lost my thyroid to it being so toxic. I requested both my gp records and hospital records, I was horrified to see several below and suppressed TSH and only one of these results contained a T3 test which they said was normal, out of about 5 TSH 2 had SEE DOCTOR! at no point did my doctor see me about those results! Forward to 2019 after surgery I was put on T4 I did not get along with it and after some time found out it contained lactose, I'm lactose intolerant! They tried me on T4 lactose free then found out I was not absorbing it to well, I have colitis it was on my tummy to long, anyway after a lot of to and frow my endo eventually prescribed T3 lactose free, I've been tolorateing this quite well going up slowly, since going on it, Other endos have tried to get me off it, also my doctor as tried to put me back on T4 several times, yes it's a cost thing, but this is no excuse if your doing well on it, I have an appointment with a gp on Monday and I know they are going to try to get me off it again as they received a letter from my endo saying he recommends I come off T3 as it's not working for me, it clearly is as my TSH as come down from 19.32 to 14.3..i feel I know more about these conditions than any doctor or endo it's embarrassing how little they actually know.. And also they are diabetes specialists first and thyroid specialist second..
Hi josephineinamachine❤️You know what angers me the most is if my gp had just listened to me and actually looked at me instead of looking at blood results and ignoring them, I lost over 2 stone in weight and he either never noticed or never cared, and I was a size 12 before hyperthyroidism went to a size 6 I was like a skeleton that in my mind is not a good doctor!! Having somewhat a similar problem with hyperparathyroidism, they know my calcium is high my parathyroid hormone is high but still they were dragging their feet, well I've managed to get an appointment with an endo but its in July 😠.. In the meantime I've to watch my symptoms, what a caring bunch they are.... NOT!!! ❤️❤️❤️❤️
So sorry to gear this Birkie......there is much ignorance among GPs and the so called specialist out there about thyroid. If the GP or Endo tries to take you off a treatment that is working they are incompetant. If it happens Id follow it up with a letter to the practise manager stating you feel removing it will cause harm to you and you want to know what treatment they will offer you which is effective as levothyroxine did not work and you fear it will cause you harm. Ask them to respond is a specified period of time.
Hi waveylines❤️Yes my gp recived a letter from my endo in Newcastle he recommends I come off T3 as its not working for me, my TSH was 19.32, I have steadily increased the T3 meds and my TSH is now 14.5, I'm due blood work next week so I will see what my levels are, not to bother about the TSH I'm more interested in my T3 level, given I've not faired to well on T4, proven by my blood work (not absorbing) I have colitis so it's not to good for a table to sit to long on my stomach hence the other endo prescribing T3, faster acting, if they do try to remove the T3 I will demand NDT, as I'm never going back on T4, see how they like them apples, 😊
-Assuming both policies align provided your mother is willing & even confirms you are authorised to represent her. Or she wishes to do this on her own or together with you . You can challenge her GP’s perception /understanding & present him with a printout Of both. But be careful because even if a referral is made there is a get out clause for both the FO & an endocrinologist. An Endo does not have to follow the NHSE/RMOC guidance at the personal level & the GP if lacking experience can object to tasking over prescription after a successful trial of T3 if he/she feels it is too complex/uncertain for him/her to be confident in managing this even with Endo oversight. Hard to understand but that’s the situation. So if you get referral (and NB, this applies just as much to private consultancy) do make enquires as to the Endo’s stance on T3. One way suggested by those who have done this, is to make a phone call to the Endo’s secretary & ask point blank whether the particular Endo is prepared to consider a T3trial. Do not be fobbed off on this point!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
