My consultant thinks this is subclinical hyperthyroid. I have had hashi hypo for at least 17 years - probably 23. I now have problems with my heart (tachycardia, probably cortisol spikes taking it to 150bpm, and sudden drop offs to 33bpm, but I can't tell this is happening).
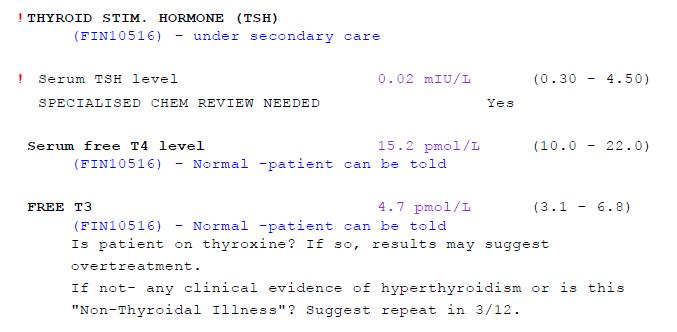
I take 3 grains of NDT and 100mcg of synthetic T4 as I am a bit resistant. This treatment puts T4 and T3 in the normal bracket (see recent blood test).
If I reduce the dose, the T4 and T3 levels drop to the the bottom of range, or below. How can I get my TSH normal, and keep both my T4 and T3 normal?
I have had problems converting T4 to T3 in the past but this was probably due to untreated Lyme disease, which I think has been halted although it has left damage.
What am I missing / not seeing???? When I first started this treatment I was advised that taking T3 (synthetic or naturally via NDT) would supress my TSH.
Any help would be most appreciated.
Written by
Confoozled
To view profiles and participate in discussions please or .
Well, a good start would be to find a consultant who knows what they’re talking about.
How on earth have they concluded you have subclinical hyperthyroidism? You take T3 containing thyroid hormone replacement—of course your TSH is suppressed! Arrgghh, this stuff makes me so cross. Why don’t they get it??
Suspect your consultant is a diabetes specialist who’s completely out of their depth.
Those latest results show you to be slightly undermedicated (given you have symptoms).
And you probably won’t be able to get your TSH into the normal range—when you’ve been on T3 containing meds for a while it sometimes messes with TSH permanently—the pituitary just seems to stop bothering making it (or rather, not a lot of it). So you’ll be on a hiding to nothing reducing your dose trying to get your TSH into range—all it’ll do is leave you feeling worse than ever.
He said as 'I'm involved with my treatment, e.g. I want to take NDT, I have to take responsibility for it" e.g. dying because of hyperthyrotoxicosis caused by my own stupidity of not using T4 only.
I needed to speak to other people as he's got me terrified and stressed.
You're not alone , and it's not just with NDT, i've ben told by Gp that , i quote "You'll Die" I was on 112.5 Levo at the time , and am on that dose again now , (but bloods are quite different for no apparent reason)
P.s ... i'm not dead yet.. i think he had just had run out of 'fob off' answers when someone knew enough to question his reasoning.
i've decided to keep him as My GP for now , just to annoy him by not dying as instructed.
This is all a bit complicated for me at times but even I know that doctors don't put you on Levothyroxine for sub-clinical hypothyroidism. I'd get a second opinion and ask the endocrinologist to explain themselves as they don't know what they're talking about.
you probably won’t be able to get your TSH into the normal range—when you’ve been on T3 containing meds for a while it sometimes messes with TSH permanently—the pituitary just seems to stop bothering making it (or rather, not a lot of it). So you’ll be on a hiding to nothing reducing your dose trying to get your TSH into range—all it’ll do is leave you feeling worse than ever.
Dear god in heaven, how on earth doesn't he know that?
Hello I need clarification. I thought if your TSH level is low, in other words going down then that’s more optimum than it having a higher number. IE. .5 TSH is more optimum than 1.5.
Second, I am taking 15 Mcg of T3 level Levothyroxine , and 25 Mcg of unithyrod
Are you saying that with my dosage, then this is going to Prevent my pituitary gland from ever from really regulating my TSH level ? Because of taking the Levothyroxine??
Essential to test vitamin D, folate, ferritin and B12 too
What vitamin supplements are you currently taking
Are you on absolutely strictly gluten free diet
Was this test done as early as possible in morning before eating or drinking anything other than water
Last dose levothyroxine dose 24 hours before test
If/when also on T3, or NDT make sure to take last third or quarter of daily dose 8-12 hours prior to test, even if this means adjusting time or splitting of dose day before test
I have no idea where to get any of those tests. I can 100% guarantee you it won't be from my NHS docs. Do you have a lab you use?
Wellwoman Max, Q10, extra D3
Mostly gluten free. Although I'm going back to that as it does have an impact on me. Also I as taking curcumin C3 - very good so I'm going back on that as well. Brilliant anti-inflammatory.
A bit of my answer disappeared. I am rigid on my tests - no meds for 24 hours and before 10.00am on an empty stomach. If I forget - I call up and rebook.
Thousands of posts on here with private testing results
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested. Also EXTREMELY important to test vitamin D, folate, ferritin and B12
Low vitamin levels are extremely common, especially if you have autoimmune thyroid disease (Hashimoto's) diagnosed by raised Thyroid antibodies
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
Last dose of Levothyroxine 24 hours prior to blood test. (taking delayed dose immediately after blood draw).
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
If/when also on T3, or NDT make sure to take last third or quarter of daily dose 8-12 hours prior to test, even if this means adjusting time or splitting of dose day before test
Is this how you do your tests?
Private tests are available as NHS currently rarely tests Ft3 or thyroid antibodies or all relevant vitamins
Leaving 24 hours since your last dose will give false low numbers, especially for fT3 which will be about 40% too low if you take your tablets once a day. More if you split the doses. Your fT4 of 15.2 is strange for someone on 100 mcg levothyroxine plus 3 grains, it would suggest an interval greater than 24 hours or poor absorption. In any event your TSH is low because of your high hormone intake.
You may need this dose to be well but it is possible this dose is causing your cardiac problems. It’s also possible the heart problems have some other cause. If your heart issue resolves when you are on a reduced dose you have the answer.
Some patients need high doses of thyroid hormone but this can cause cardiac problems. In cases like this there can be different response to thyroid hormone in different organs and the heart usually seems to be more sensitive. For the patient this means they have to compromise on their dose and perhaps try to protect the heart with a beta blocker. In the longer term I feel patients and doctors need to adopt better science and find out why this happens.
It is wrong (and dangerous) to assert ‘T3 always suppresses TSH’. It depends on the dose pubmed.ncbi.nlm.nih.gov/204... . TSH becomes too low either because the pituitary is under performing or a high T3 dose suppresses TSH. If a high dose is taken for a long time it can down regulate the hypothalamic pituitary thyroid axis which leads to long term low TSH. We should try to avoid high doses IF possible.
I was looking at your first post "of course your TSH is suppressed" although I had in mind many posts that suggest TSH is always suppressed on T3.
I think quite a few posts were put up around the same time as mine and I didn't see them, including your later one.
It's quite likely the high doses have down regulated the axis and so TSH doesn't recover. This is why I feel it is best to try hard to get better on moderate doses but of course this isn't always possible.
If too long an interval is left between the last dose and taking the blood it will give false numbers.
Here's one that refers to using high dose levothyroxine thieme-connect.com/products... . I've seen many studies but don't have them to hand. The axis can be down-regulated by taking too much levothyroxine, liothyronine or NDT of by periods of hyperthyrodism due to autoimmune thyroiditis, Graves' etc. Sometimes the patient may not have known they were hyper.
You've posted about your experience with acquired thyroid hormone resistance, so I hope you don't mind me asking this. Did the high doses of thyroid hormones that you took suppress your TSH? If so, has it recovered?
Yes it fully supressed my TSH, I was on supra-physiological doses for about 10 years. In 2017 I tried coming off / reducing my hormone intake for a few months but was unable to restore my axis and needed about 50 mcg L-T3 + 50 mcg L-t4. Since we have another lockdown and I can't do my normal badminton / squash etc. I'm now having another try. I'm currently on 75 mcg L-T4 only and am quite tired, get back pain, have dry skin and make silly mistakes with poor concentration. I will give this a couple of months plus to see it things pick up - my thyroid is healthy.
If my axis picks up I should be fine without any need for thyoid hormone. The studies I've seen suggest the axis picks up in more than half of people after about three months, much longer if they have Graves' antibodies. A problem with these studies is they measure recovery as TSH, fT3, fT4 coming back into their reference intervals. They don't try to assess whether fT3 and fT4 become 'normal' in the sense they hover around mid-interval.
My axis has been suppressed to a greater extent and longer than most cases because it took a decade to find the underlying cause of my hypothyroidism.
My understanding is that you should have no functionality left in your thyroid after such long term suppression. Therefore how can you have no thyroid replacement or be on such low doses?
Don't know about decade plus supression. Might find out! Certainly the thyroid can recover after TSH supression for a year or two. It doesn't disappear and can recover.
The thyroid can recover but my TSH did not respond adequately to the low normal fT3, fT4. Hence my thyroid and deiodinase was insufficiently stimulated. It's probable that the pituitary produces TSH with low bioactivity when the axis is down-regulated. I conclude this from the ineffectedness of the TSH, 2.35 is not low in normal circumstances.
My results on 75 mcg L-T4 were: -
TSH 2.35 (0.27-4.2)
fT3 3.3 (3.1-6.8)
fT4 16.1 (12.0-22.0)
In cases of low hormone like this the body will attempt to conserve hormone which likely explains my fairly normal fT4. In addition my thyroid would have made a small contribution. I was hypo with substantial tiredness, back pain on walking short distances, dry skin and I can't remember what else. It was such that I couldn't continue for more than a couple of months.
The low T3 reflects poor T4 to T3 conversion. At these hormone levels type-2 diodinase dominates and this regulates local T3 in tissues that express D2 such as the brain and skeletal muscles.
Thanks for your answer. I don't know if many people would be willing to become symptomatic for the chance they might restore their axis (particularly after 10 years) and never need thyroid hormone replacement. Good luck with your experiment and recovery. It would have been interesting if you'd had cardiac and bone density tests before and after the 10 years of TSH suppression, as those are often mentioned as hazards of suppressed TSH.
The studies I've seen suggest the axis picks up in more than half of people after about three months.
That's interesting. I don't suppose you could cite a reference? I'm not questioning your assertion, just would like to understand this subject better. I think I've read here comments to the effect that a long-suppressed TSH may not ever recover.
Because TSH promotes T4 to T3 conversion, especially in organs that like to regulate their own T3 levels. TSH plays other roles such as in regulating bone turnover. The main role of TSH is to stimulate the thyroid to create and secrete thyroid hormone. It's better if you have a normal TSH but this is not always possible.
there's also a link from suppressed TSH to dementia and early death but again that depends on the group being checked - there's no differentiation I can find as to the root cause of the suppression and if that reason is linked to either dementia or early death. The early death seems to more related to cardiovascular health.
Cardiovascular damage can lead to 'low T3 syndrome' in which T3 is kept low by the body by local mechanisms and by the hypothalamus producing less TRH leading to lower TSH. I usually refer to low TSH because it is not always supressed i.e. not low because fT3 and fT4 are too high. Linking a low TSH to dementia or heart conditions is a bit too complicated to draw conclusions.
Yet there are quite a few studies that do exactly that with lip service in the methodology as to the actual reason for suppression. It's simply based on a tsh blood reading via subclinical hyperthyroidism diagnosis.
Just to add, when hypothyroid one has low metabolism and it's very common to have low stomach acid.
This in turn leads to low levels of vitamin and minerals as your body is not able to effectively break down and use the nutrients from your food. The same issue applies if hyperthyroid - and when your metabolism is running too fast - as now your body is running too fast to break down food for you to build strong levels of nutrients.
No thyroid hormone works well if ferritin, folate, B12 and vitamin D are not maintained at optimal levels and by this it is not just a question of being in a NHS ranges somewhere but being at optimal levels for you to convert T4 into T3.
T4 is a storage hormone that the body needs to be able to convert into T3 which is the active hormone that the body runs on and is is said to be about 4 times more powerful than T4 - with the average person using about 50 mcg T3 daily, just to function.
I now know I feel at my best when my ferritin is up at around 100 as my conversion of my thyroid hormone replacement is the best it's ever been :
I am self medicating with NDT which contains approximately 9 mcg. T3 + 38 mcg T4 per grain/tablet and i dose to the relief of symptoms and not a blood test and certainly not a TSH level.
I understand very few of the medical profession know how to treat with NDT and revert to what they know which is generally how to treat and monitor with Levothyroxine and it all gets confusing as medics need to work within the medical guidelines and legal framework the their professional medical insurance.
T3 - is a hormone produced by the thyroid - and commonly referred to as synthetic Liothyronine just asT4 - another hormone produced by the thyroid is commonly referred to as synthetic Levothyroxine.
Yes, years ago before the science of blood tests people who were thought to be hypothyroid were given a little bit of pig thyroid to chew on.
At follow up - if symptoms were gone - the doctor was considered amazing and another slither sliced :
if symptoms persisted, a larger nugget would be dispensed, so forth and so on until the patient felt better, and doctor became richer.
I think Big Pharma rolled out synthetic T3 and T4 in around the middle of the last century when medicine became more of a capital venture and bottom line business.
But taking T3 in a small dose such as 10 mcg daily can also provide the same type of suppression in TSH. I had that happen to me when I was first introduced to T3 along with T4. Have no idea what would happen to the TSH number if I ever stopped T3 but at the moment certainly do not want to try it. I am good right where I'm at even though my TSH is at .02 and has been since 2016🙂
Have you addressed the Lyme disease? Often times people who have had Lyme disease have problems with viruses eg EBV (glandular fever virus which hangs around); herpes viruses (not just the ones that cause cold sores) coxsackie virus etc. I found treating all those combined with making sure my B vitamins and D vitamin, zinc, selenium, magnesium as well as reducing liver inflammation really helped with better absorption of thyroid hormones.
You have some excellent advice from others so I wish you well.
I did 4 weeks of doxycycline at 400mcg. Absolute turning point. Of course had to source and treat it myself based on a very intelligent patient comment i read about why and how. Thank you for your observations on Lyme. I'm going to do the blue horizon test I think as I have no vitamin baseline.
Doxycycline will help with bacterial infection (borellia) but it won’t kill off viruses. I used high dose pantethine and l lysine. I also used a herbal anti viral concoction. With some Lyme patients it’s the viruses that are just as problematic as the bacteria.
Also if you had 4 weeks of doxycycline did you take a good probiotic? I found megasporebiotic to be the best. It’s v expensive but v good.
The doxy had a huge impact so I'm thinking it must have been heavily bacterial. I'll look at the viral side and check out the probiotic you mention. Yes i did use them at the time but I'm going back to this I think as this will be an issue.
I take levothyroxine and self medicate with liothyronine in addition. My TSH has been <0.05mIu/L (0.3-5.5 reference) every time I tested since. It wouldn’t even cross my mind to consider I may be going hyper just because my tsh is suppressed. Thankfully my GP accepts that my tsh likes being low and he never gives me any problems. Your endo sounds like someone who’s got an agenda to push you onto Levo either because of not understanding the t3 effect on tsh or deliberately misleading you.
Your current symptoms look a lot like mine...my doctor said that low cortisol will raise adrenaline levels and that can cause hyper-like symptoms like increased sweating and racing heart. The STTM talks about "T3 pooling" when T3 stays in the blood and cannot enter the cells due to cortisol dysregulation. They claim that raises adrenaline levels so it´s all about the chicken and the egg...but I am not too convinced by the STTM´s claims that T3 pooling should be treated with T3 only. If T3 cannot enter the cells due to high adrenaline and low cortisol, it shouldn´t matter if you take T3 directly or get it from T4 conversion.My FT4 levels are only midrange on 200 mcg of levo but my FT3 levels are at the top of range so not what you would expect on levo only. Which would point to T3 not getting into the cells. A 24 h urine analysis showed T4 levels slightly below range and T3 levels at the bottom of range so the doctor concluded I´m hypothyroid. It would seem I am converting T4 to T3, though, but it´s not getting into the cells. If adrenal treatment is necesssary, I´d prefer adrenal glandulars which provide support for the adrenals rather than prescription Medrol which the doctor suggested.
Blood tests showed midrange cortisol levels at 8 am but 24 h urine showed below range cortisol, hence the doctor´s conclusion I have adrenal fatigue.
I sent a link to one of your posts to my endo as I thought we had a lot of similarity. I've never heard of a urine test for t4 etc? Also I mentioned that my heart is being affected by cortisol and the endo dismissed it. But I think it is.
It´s not commonly used but ordered by anti-"hormone doctors" such as the Hertoghe doctors in Belgium and some alternative practitioners in Germany and Switzerland. Not sure about UK docs such as Drs. Skinner and Peatfield. The doctors who order 24 h urine analyses say this shows what is being available at cellular level, whereas the hormones in the blood don´t tell us much as there is no way of knowing how much actually enters the cells. They measure all hormones - thyroid, sex hormones, adrenal hormones - that way, along with vitamins and minerals, and base their prescriptions on the levels in 24 h urine rather than blood. Most doctors, especially endos, don´t recognise the existence of adrenal fatigue. It´s treated by unconventional doctors using either prescription drugs or glandulars/adrenal cortex. Most convetional docs dismiss the link between the thyroid and the adrenal glands...
Also, a few years ago when I was on levo and not feeling optimal, I had several vitamin and mineral deficiencies that my doctor at the time never discovered because no tests were ever ordered. It was with the help of this and other forums that I ordered private tests and started self-treating mineral and vitamin deficiencies. I now take vit D daily (no longer just during the winter months) along with a good vit B complex, high doses of vit C, zinc, selenium, magnesium, and I have also managed to get my iron and vit A levels up by eating black pudding once a week. It would seem my body is now more able to convert T4 to T3 than before so my own experience is that optimal vitamin and mineral levels are crucial for thyroid patients. I am not saying it will be enough for everyone, but it seems to have made a hugh difference to how my body now uses levo.
I remember reading a study from the 1940s which found higher than average vits are required by hypos. What you write is like a case study of that research done 80 years ago and utterly ignored by the medical community.
PS. The reason they suggest you are overtreated is because your TSH is below range. Most doctors including endos only care about the TSH and, even if they check your free Ts, they have no idea how to interpret them. Your free Ts are well within range so you are absolutely not overtreated.
You are undermedicated. Both FT4/3 at around 43% through range. TSH will be suppressed when you supplement with T3.
The argument that TSH plays a role in conversion is a mute point when the bloomin conversion isn’t happening regardless of what level the TSH is.
You are in now way near to hyperthyroid and if you have the energy then make a complaint but if energy is difficult to find then use whatever you have to find a new Endo because this current one is a dud!
I have also always wondered about the TSH and its role in conversion...I have been unable to keep my TSH in range even on levo. Every time I felt good, my TSH was below 0. When I was on 150 mcg levo my TSH was 0.09 and I felt much better but was told I was overmedicated and levo was reduced to 125 mcg...after eight weeks, my TSH had gone up to 7 and the doctor said that was preferable to a very low TSH...the TSH has never done anything for me. My TSH ended up <0.01 on 200 mcg of levo. Judging from my symptoms in the past couple of years, I had a few Hashi swings before my thyroid finally gave up...for some reason, I ended up feeling very overmedicated and had to go off levo for a while, felt good for about eight weeks before symptoms returned and then I went back on levo...of course, Hashi swings can suppress the TSH just like Graves can. After about six weeks off levo, my FT3 levels were still slightly out of range last year which makes me suspect a Hashi swing. It would seem that once the TSH has been suppressed for some time, it may never normalise so that should not be the goal. My TSH has never, ever coincided with my symptoms...when doctors told me I was optimally treated (based on the TSH), I felt horrible because of low free Ts, and when I felt fine I was told I was overmedicated and had to cut back...I gave up on doctors a long time ago.
I have been the same, 10yrs of my GP treating my Hashi’s by TSH results meant that I was forever on a rollercoaster and living life standing behind a half closed door! As soon as added T3 my TSH went to 0.005 and has stayed there. I did some conversion but very poorly so that my FT3 was always about 0% through range but as far as my GP was concerned it was ‘in range’ so no problem.
There’s no point in ‘allowing’ or trying to stimulate conversion (by allowing TSH to sit in range) if the job that’s being done just isn’t adequate. So for me TSH is about as useful as a chocolate teapot, the studies that show TSH role in thyriod health are not helpful, it may be a fact but it’s a useless one to many of us who are being held in a state of half life because of TSH results.
We need to get back to listening and believing patients.
Even now my private Endo is trying to treat me based on blood results with some disregard to how I feel. How is it ok to think that 3.5 is ok but 6.5 is not? Range (3.5-6.5) it doesn’t make sense.
Endocrinologists in my experience have zero interest in the overall wellness and functional ability of patients. If you're crawling on the floor unable to do anything but the most basic tasks that's good enough for them.
I've read studies where Endos sneer at patients, and these comments have been published as part of academic articles, for asking for help to return to wellness. The contempt for the patient and arrogance of the doctor are beyond comprehension.
I asked the Endo about this multiple times e.g. 1) Is he interested in my overall wellness or just the TSH result 2) what happens after he's 'fixed' the bloods to normal TSH and t4/t3 allegedly in range. Will he follow up to see how I'm faring or just hand me to a GP to manage feeling his job is done and my wellness is no longer his concern. He refused to answer.
I spoke to a GP once who asked me why I was different to the more than 200 serious endo patients he'd treated over 20 years in practice. He said he watched each one steadily decline so why was I different . The answer is I was following a combination treatment and not TSH only management. So clearly GPs treat patients according to NICE guidelines but these have zero interest in helping the patient return to a quality of life experienced by the average person and focus on a mediocre programme of 'it's good enough for them'.
My GP said ‘why are you different to the other thyriod patients I treat?’ What they meant by this is ‘your in range numbers are no different to my other patients but they are not bothering me every few months, whining like a little b**ch, why aren’t you grateful for some relief like they are?’
This was some years ago and at the time I remember feeling like I was the problem, not the treatment. I went away and tried to be grateful, I just didn’t have the energy or the mental health. Back and forth I went, it was exhausting! Each time my GP tried to pin Fibromyalgia and bi-polar on me. I declined their offer of fobbing me off.
Confoozled, I’ll eat my hat if you’re not under-medicated. Your FT3 is just not optimal for you. I hope you find a way forward 🤗
I think one problem with endos is that most are not thyroid specialists but specialise in diabetes. They take diabetes very seriously but consider thyroid disease, especially Hashimotos, unworthy of their attention. To them, it´s easily treated with levo and once your TSH is anywhere in range you are fine. Remaining symptoms are not related to your thyroid condition. Period.There is one blog called HormonesDemystified where the owner claims to be an endocrinologist. I have no idea if it´s true, but this guy is completely anti-T3. He claims that the reason people initially feel better when they add T3 is because of its stimulating effect...basically concluding people on T3 or NDT are drug addicts. He also ridicules people who believe that NDT is natural because its T3/T4 hormone ratio is very different from that in humans, concluding (and I quote): "That is fine if you are a hypothyroid pig"...
He phoned me up and told me I'm going to die from thyrotoxic biochemistry because of my meds. And die imminently.
The man is an idiot, and a disgustingly callous one at that. If you died from taking NDT and Levo, you'd be the first person taking NDT to die as a result of taking it since records began in 1967, and only the 20th person to die as a result of taking Levo, also since records began in 1967.
Compare that to people who die as a result of taking statins, diuretics, blood pressure meds, blood thinners etc, and Levo is much, much, MUCH safer than all of them.
You can view adverse effects data of most or all drugs prescribed in the UK plus some that are over-the-counter on the Yellow Card site, run by the MHRA.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.