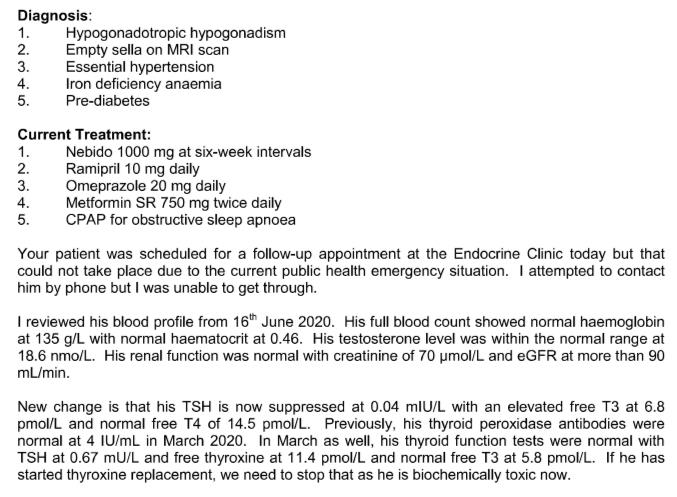
Today I seem to be posting for other people not myself but this is important to me so here goes . My husband has just received this message from his consultant endocrinologist today.
Biochemically toxic - can this be true ? - Thyroid UK
Biochemically toxic - can this be true ?
Written by

Steni
To view profiles and participate in discussions please or .
27 Replies
•
Difficult to say without the ranges. But, I somehow doubt it. FT3 doesn't look that high.
PurpleNailsAdministrator
If he has started thyroxine..... doesn’t the doctor know? If his results were all normal in March, what would be the reason?
Did he start medication? FT3 elevated, but it doesn’t look very high. Do you know the range?
The doctor doesn’t know ! It’s some crazy situation that’s come about - I’ve asked him to get onto the hospital and get the ranges for these tests.
If he was taking levothyroxine his fT4 would be high. Is he taking any other form of thyroid hormone or supplement? If not possibly he has thyroiditis. I would look at any other medication he is on in case of side effects.
He is taking 100mg Levo as advised by his gp
The consultant should have said he was thyrotoxic not 'biochemically toxic'. This doesn't inspire confidence. Thyrotoxic is a little over the top given your husband's fT3 is a little high and his fT4 fine.
The levothyroxine would not have caused his high fT3 because fT4 is a little low in interval. It would help to reduce or possibly stop the levo but levo is definitely not the cause of the high fT3. It's most likely your husband has some form of thyroiditis that is causing the thyroid to secrete too much T3. Rarely another illness can affect the thyroid or T4 to T3 conversion.
If his fT3 remains high the consultant should consider 'block and replace', giving e.g. carbimazole to suppress the thyroid and replacing it with levothyroxine, this gives stable hormone levels. The fT3 may settle down by itself or more likely rise and fall over time until the thyroid packs in.
Taking levothyroxine is not the cause of the high fT3. It's appropriate to reduce the levo, not sure about stopping it completely, maybe he could discuss with his GP. The consultant could have been more helpful. If they have sufficient knowledge that is!
SlowDragonAdministrator
Is he taking any thyroid medication? Levothyroxine, NDT or T3?
Has he had BOTH Tpo and TG antibodies tested
What vitamin supplements is he taking?
He’s taking Levo 100 / no supplements ?
Realise this is an old post
On levothyroxine we need OPTIMAL Vitamin levels
Metaformin lowers B12+
As he’s taking metaformin it’s likely he will need to supplement B12
Low iron/ferritin need improving to optimal
Just testing TPO antibodies is inadequate. Need to test Thyroglobulin antibodies too at least once
For full Thyroid evaluation your husband needs TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested. Also EXTREMELY important to test vitamin D, folate, ferritin and B12
Low vitamin levels are extremely common, especially if have autoimmune thyroid disease (Hashimoto's) diagnosed by raised Thyroid antibodies ......or if under medicated
As he has pituitary problem it’s always essential to test TSH, Ft4 and Ft3
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
Last dose of Levothyroxine 24 hours prior to blood test. (taking delayed dose immediately after blood draw).
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or thyroid antibodies or all relevant vitamins
List of private testing options
thyroiduk.org/getting-a-dia...
Medichecks Thyroid plus antibodies and vitamins
medichecks.com/products/adv...
Thriva Thyroid plus antibodies and vitamins By DIY fingerpick test
Thriva also offer just vitamin testing
Blue Horizon Thyroid Premium Gold includes antibodies, cortisol and vitamins by DIY fingerprick test
bluehorizonbloodtests.co.uk...
If you can get GP to test vitamins and antibodies then cheapest option for just TSH, FT4 and FT3
£29 (via NHS private service ) and 10% off down to £26.10 if go on thyroid uk for code
thyroiduk.org/getting-a-dia...
Also vitamin D available as separate test via MMH
Or alternative Vitamin D NHS postal kit
Come back with new post once he gets results
helvellaAdministrator
Even if that FT3 were a little high (and the TSH a little low), it would be inappropriate just to stop, cold, without the doctor even knowing what dose he might be on.
Example:
He is taking a significant dose of thyroid hormone (whether levothyroxine or liothyronine or both). That would have had the obvious impact on the thyroid tests. It is not impossible a small adjustment could be required. If he were on, say 150 micrograms, maybe 125 or 137.5? But drop to zero is an unthinking reaction which would have the effect of pitching him straight into being significantly hypothyroid.
Like seeing a red traffic light ahead and immediately doing an emergency stop. Though it is a straight road and the lights are a mile away.
The t3 level is not drastically high for someone on NDT or t3 .... however, if he isn't taking any thyroid replacement it'd be unusual and suggests his thyroid is flaring up. I'd be concerned about his vitamin and mineral levels, especially since he's on PPIs and metformin.
Firstly may I ask if your husband is overweight? Pre-diabetic and sleep apnoea tend to suggest he might be. If so, might he consider losing weight? I presume he's taking the omeprazole because all the other drugs are giving him gastro-intestinal issues.
But. Why is his anaemia not being treated? If he can't tolerate tablets, I'd suggest he considers Spatone (sachets of iron rich water) and/or iron patches such as those available from Patch MD. (You can buy both of these from Amazon).
As for biochemically toxic, just because his Free T3 is slightly above range. No repeatable comment. His FT4 and FT3 don't seem to match for someone who is on Levo. He seems to convert T4 to T3 well, so maybe try reducing to 75mcg levo and see if he feels better or worse. You can just do this yourself at home for a few days to see what happens (at least that's what I would do).
Thank you so much for your reply . I too thought it was an extraordinary comment !
Re your other points it would certainly be wonderful if he would lose weight but he craves and then gives into longing for sugar - his consumption of sugar is very high. He tells me just now that he is having some iron tablets so I guess that is now testing the anaemia . None seems to know why he is anaemic in the first place and have investigated the possibility of an internal bleed many times with no result.
What would be the purpose of dropping down the Levo if it’s isn’t responsible for the high T3 ?
My thinking behind reducing the levo is that he appears to be converting too much T4 to T3. If he takes less T4 then his FT3 level might come down a bit.
Anaemia is pants - I know, I've had severe anaemia in the past. If he can get his anaemia under control he might feel better. If he struggles with the tablets, he can consider trying the things I mentioned above, which are gentler on the insides. Many people get constipation on iron tablets. I had to be different - for me it felt and acted like swallowing a Brillo pad!!!
He needs to get his sugar craving under control, if possible. I use pure stevia to sweeten things at home. You have to shop carefully to get the real thing, not mixed with something else.
(All just suggestions, I have no qualifications at all, just experience.)
Looking at your reply below about his pituitary, I would also consider if he might have adrenal problems. Sugar craving could, possibly, indicate that he might. The adrenals are also controlled by the pituitary.
To test adrenals, consider the saliva cortisol test - you can order it via the thyroid UK website. Does he find he gets stressed easily or feels anxious? I'm just wondering if adrenal cocktails might help him - google it to be certain of the ingredients as I'm typing off the top of my head here - but I think it's orange juice, salt (I use celtic sea salt, but Himalayan also works) and cream of tartar. It can work like a charm in just a few minutes - or make no difference at all.
Biochemically toxic just means over medicated rather than from a physiological cause. However I see your husband has empty sella so he potentially has central hypothyroidism due to a failure of the pituitary. If this is so then TSH is meaningless and thyroid function should be entirely on ft3 and ft4. I think your husband needs to go more on symptoms as well as blood tests. Does he feel well?
What does Empty Sella mean ? Excuse ignorance
This link has detailed and good information:
Seems obvious to me his T3 is pooling due to his iron deficiency anemia. His T4 is normal. The medications he is on are usually due to badly managed hypothyroidism. If I was you I would get the anemia treated and then look into his blood sugar levels. Lack of stomach acid too by looks of things and then they go give him omerprazole and make his stomach acid even less. If they are saying pre diabetes I would give the thyroxine a chance before you dive in to the metaformin. Hypertension too also could be due to hypothyroidism. Sleep apnea also due to hypothyroidism and lack of vitamin D. So overall I would be questioning all the medication to cover up what could be due to him being hypo. Needs to have the anemia fixed then hopefully everything else will fall into place and he can get off all those awful medications.
Yes they are saying that he is at the Pre diabetes stage and yes he is taking metformin. How long after getting the anaemia fixed could he drop the other meds ?
I agree with what is being said about hormones. I'm going through the same right now and my cortisol and dhea low. Turns out all my hormones are low. It would depend on how well your husband responds to treatment and how long it takes for the T3 to get into his cells. You have also got to convince his doctor to look again at the overall picture. Doctors are not good at that. Hopefully once his thyroid settles his blood sugar etc will normalise. You will have to convince the doctor too to wean him off all these medications.
Empty sella suggests central hypo, so TSH should be being ignored. No ranges, but FT3 looks like top of range, and FT4 low in range, but I wouldn't be concerned unless hyper symptoms and anyway, that would just mean a small decrease in dose. not stopping levo completely. I read somewhere that metformin could affect some test results
Yes Metformin lowers B12 ..
Ok so no worries about TSH then ?
stopthethyroidmadness.com/i...
Ok, so he's already diagnosed with hypothyroidism. Therefore, his cortisol and dhea should be checked. Low cortisol and iron deficiency aneamia combined is possibly keeping t3 in the serum (blood) and out of his cells (t3 pooling) according to the link above.
As his pituitary is currently shown to be in an atrophied state, it's essential the endocrinologist doesn't ignore adrenal hormones (he already has low testosterone and thyroid). Some people on the forum take hormones like pregnenolone and hydrocortisone to help with low cortisol and dhea, but it'd probably be worth asking a bit more (new post) about pituitary issues as it's not my area really. He'll definitely need vitamin D levels checked and in order to make adrenal hormones he'll also benefit from magnesium (helps uptake of Vitamin D and stops insulin resistance), zinc, chromium (regulates blood glucose) and b vitamins (b12 could be low due to his meds and low stomach acid) and lots of Vitamin C.
Fantastic advice - thank you so so much. We’ve learnt more today than I the last year!
Not what you're looking for?
You may also like...
Is this true
I'm new on here even though I've been diagnosed as hypothyroid 16 years ago.
I've just asked my...
Can this still be my thyroid?
Hi everyone
Just at a very low ebb this evening and looking for some advice. I was diagnosed with...
Is this true ?
I found an old blacks Medical dictionary in a second hand shop and looked up Thyroid (as you would)...
Biochemically euthyroid with symptoms??!
Hey, I was wondering if anyone had been through this and could give me some advice. I was diagnosed...
HELP - HOW CAN THIS BE?
Okay - on T3 only and been doing well since 2012. BUT.. for the past 6 months tsh has been...