Hi lovely people - I’m hoping you can kindly advise me again on my results. I’m advised my Vit D is still low - I seem to having trouble getting this to improve.
I feel nauseous a lot of the time (gastric problems too) - it maybe unrelated to thyroid ( I take 75mg) and wheat products make me feel worse.
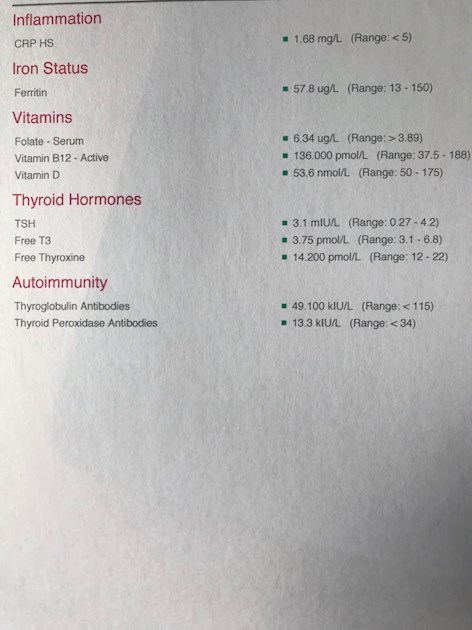
Here are my results from medichecks. I’m endeavouring to remember to take the vit D at supper time (an oil).
Huge thanks for any help. X
Written by
Scullngbunny
To view profiles and participate in discussions please or .
I too had difficulty raising my Vit D levels, I changed to Better You oral spray Vit D +K2, this was the only thing that raised my levels significantly I took 3000iu daily for 3 months and got my Vit d up to 90. I dropped back to 2000iu per day but my levels fell again so I take 3000iu daily and I test every 6 months to ensure I am not having too much.
It is a little more expensive than many others forms but if you are having problems absorbing the Vit D using tablets ( I have low stomach acid which makes absorbing all sorts of things difficult) it might help to boost your levels.
Also it is advised that you take magnesium alongside Vit D ( as well as K2) as they help your body to direct the calcium in your body to your teeth and bones and away from the sort tissues.
"Also it is advised that you take magnesium alongside Vit D ( as well as K2) as they help your body to direct the calcium in your body to your teeth and bones and away from the sort tissues."
Can I just clarify that.
K2-mk7 directs calcium to bones and teeth.
Magnesium helps the body activate D3, it convert D3 into it's active form so that the body can use it.
Can you kindly advise/translate my other results - i really can’t fathom them? Do I have auto-immune thyroid problem? I’m so confused & brain not functioning properly.
Ferritin is low. It's said that for thyroid hormone to work properly (that's our own as well as replacement hormone) ferritin needs to be at least 70, preferably half way through range.
You can help raise your level by eating liver regularly, maximum 200g per week due to it's high Vit A content, also liver pate, black pudding, and including lots of iron rich foods in your diet
Folate, although over the low level, is low. It's difficult when there's not a proper range, but I'd certainly want mine into double figures. Eat folate rich foods, and consider a good quality B Complex containing methylfolate not folic acid. Most B Complex supplements contain B12 but you don't need much as you already have a good level.
I am currently using a whole food B Complex containing 400mcg methylfolate but only 24mcg B12 as my B12 level is very good.
The Vit D Council recommends a level of 125nmol/L (50ng/ml) and the Vit D Society recommends a level of 100-150nmol/L (40-60ng/ml).
To reach the recommended level from your current level, based on the Vit D Council's suggestions you could supplement with 3,700iu D3 daily (nearest is 4,000iu)
When you've reached the recommended level then you'll need a maintenance dose to keep it there, which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. You can do this with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
D3 aids absorption of calcium from food and K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking tablets/capsules/softgels, no necessity if using an oral spray
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking tablets/capsules, no necessity if using topical forms of magnesium.
Check out the other cofactors too (some of which can be obtained from food).
**
Don't start all supplements at the same time. Start with one, leave it 1-2 weeks and if no adverse reaction then add the second one. Continue like this. If you have any reaction then you will know what caused it.
**
Your thyroid results aren't much better than when you posted 3 months ago. You need an increase in your dose, 25mcg now and retest in 6-8 weeks.
Did you ditch the Teva brand?
**
Do I have auto-immune thyroid problem?
Your antibody results are below the limits so technically negative. However, they're not exactly very low so I wouldn't be surprised if you do actually have Hashi's.
Considering that you have said
I feel nauseous a lot of the time (gastric problems too) - it maybe unrelated to thyroid ( I take 75mg) and wheat products make me feel worse.
also makes me think you may have Hashi's.
Are you gluten free as you know that wheat products makes you worse?
As there is a possibility of Hashi's, an oral spray is recommended for best absorption (eg BetterYou).
I’m endeavouring to remember to take the vit D at supper time (an oil).
Is this sublingual?
You need to take your D3 regularly to raise your level. Sublingual liquid/oil should be fine when Hashi's is present, but you might want to try the BetterYou spray to see if that suits you better.
Raising ferritin level could help because fatigue is one symptom of low ferritin. But I think possibly your biggest problem is that you are undermedicated. You really do need that increase in Levo immediately to bring your TSH down and raise your FT4 which will then hopefully raise your FT3.
Use the following information in support of your request for an increase in dose:
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor.
You can also refer to NHS Leeds Teaching Hospitals who say
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")