Thanks, Sue! Will have to figure out how to change picture Sorry! Unbelievable that a professor for neurology gets this wrong. Just keep fingers crossed it works at a low dose. Wonder why he did not mention PLMD on report neither!?
On drugs.com under “prescriber information”, it states the max daily dose is 600mg and the max single dose as 300mg. So, 300mg 2x/day is the maximum dose. This is in the US. Britain may have different prescriber guidelines.
OK I see that under the tabular view. Also somehow the other study I listed doesn't show and it show two of the link that doesn't work for you. And I no longer have that link. Oh well. The point was made that one can take 450 mg at one time for RLS.
Again - nothing about RLS and no general statement for all conditions of max single dose of 300 mg. Just gives for specific conditions which generally are conditions that affect the patient all day so it makes sense to divide the dose, but for RLS the need is generally only at night.
Sadly I'm not in the least bit surprised. Most neurologists know very little about RLS or PLMD.However, as the treatment is the same, the medication will work on both.
He hasn't got the starting dose or continuing dose right either.
Although NHS & NICE CKS guidelines are already out of date, they do mention a higher starting dose of pregabalin.
75mg to start and then increasing by 25mg every few days up to 300mg. As pregabalin takes about 2 to 3 weeks to be fully effective, it's better to stay at 150/200mg for a few weeks as that is the average effective dose and you may not need to go up to 300 or 450mg.
Mayo algorithm has 450mg as max. dose for RLS/PLMD.
If I were you, I'd print off the Mayo algorithm and the NICE and NHS guidelines and ask for 150mg dose for next 2 to 3 weeks, starting at 75mg and adding 25mg every few days.
It's so frustrating that neurologists don't know how to treat this common disease effectively
I’d just add that from my reading on drugs.com, USA, the “2-3 weeks” is in regards to achieving pain control. Having taken Pregabalin for PLMD, it worked the first night at 225mg at bedtime then after about 7-8 months, we increased to 300mg @ bedtime - “bedtime” as my daytime PLMW is no longer a problem. If it was still happening during the day, I’d ask for the extended release formulation.
As a long term taker of pregabalin, my advice would be to go slowly. The first few months/year likely requires dose adjustments. If a dose is working for you - even a very low dose, stick with it until it doesn't work for several nights and then adjust upwards.Pregabalin (like many medications) has significant side effects, some of which for me have emerged the longer I have been on it. That said, it works well to control my PLMD.
The side effects of pregabalin that i experience are reduced / slowed cognitive function; general spaced-out feeling; difficulty waking up and considerable morning sedation; slightly blunted emotions; forgetting words. I also have considerable daytime fatigue lasting 2 or 3 hours. And more recently my vision has deteriorated considerably (not just an age-related phenomenon). I have been taking pregabalin for approx 8 years. I have been on a dose of 300mg nightly for approx 5 years.
I am also interested in your side effects from Pregabelin. I am seeing my neurologist in a couple of weeks and am interested in what other people experience. I am suffering from loss of mental sharpness in particular.
The side effects of pregabalin that i experience are reduced / slowed cognitive function; general spaced-out feeling; difficulty waking up and considerable morning sedation; slightly blunted emotions; forgetting words. I also have considerable daytime fatigue lasting 2 or 3 hours. And more recently my vision has deteriorated considerably (not just an age-related phenomenon). I have been taking pregabalin for approx 8 years. I have been on a dose of 300mg nightly for approx 5 years.
I have done those many years. Not really helped much. No caffeine in the afternoon and no late meal helps a little, but not enough to get quality in life, i.e. be able to go to the movies etc. I have never been driving alcohol and never smoked.
The first line treatment for RLS/PLMD is gabapentin or lyrica. Those don't help everyone but a whole lot of us. They both reduce (may not be the best medical term) glutamate. Glutamate is in almost all food but is especially high in some like aged cheeses (think Parmesan, etc.), tomatoes and walnuts. Google it; these diets are the ones that epileptics pay attention to. MSG is hidden in many prepared foods in the form of "natural flavors". I avoid all prepared foods that have additives, that means emulsifiers like in ice cream, etc. I suffered with shaky legs for years before I changed my diet. Dr. B never mentioned this and I traveled twice to see him.
Oh, and all foods with umami flavor; ripe foods also have more glutamate (so less ripe tomatoes earlier in the day are okay for me, for instance). Yes, for me it means eating out (except mostly Indian and Mediterranean cuisine) is difficult, as well as eating socially where I can't know what is in things. I know we are not all the same, but those of us who respond to gabapentin, lyrica are responding to our glutamate levels being lowered. There are many websites about high glutamate foods.
Thanks. And am I correct in thinking you were taking 300 mg of pregabalin and now on 150 mg?If so, is it because of the low glutamate diet that you have been able to reduce your dose? And are you taking any other medication?
Looking back at my records, it seems I was increasing (very ironically) pregabalin in order to help with sleep maintenance. At 300mg. I was having bad side effects. I cannot tell from my haphazard records exactly when I figured out the glutamate thing and changed my diet (and started looking for other triggers, like additives, taking hints from the paleo diet helping epileptics). My biggest regret is not staying with lower doses (I am still trying to get down from 125mg where I am now to deal with sedation). 50mg. of pregabalin helped me from day one and I stupidly thought it would solve all of my sleep issues, not simply PLMD. I think the answer to your question is more or less yes. Before pregabalin I was suicidal; now I am not, but daytime sedation is 1/2 a life.
Have you tried being very careful about food/drink triggers including high glutamate (especially after 3pm)?
A final note is that I goofed by thinking some pill would be a magic bullet, not realizing that at 75 years old my sleep was not going to be what it had been in my youth. Sleep maintenance and other insomnia issues seem to be a part of normal aging, if my friends are any example.
Yes, in addition to having adopted a more healthful diet, i have been slowly moving towards a low-glutamate diet. I started with cutting out all the known high glutamate foods, and am now looking to reduce all other free glutamate sources. It's amazing that 50mg of pregabalin helped you (initially). Hopefully you can get back to that point!
You may already know that riper food (like aged cheeses and tomatoes) that have glutamate have more when they are ripe. It seems that the more flavor a food has, the more glutamate, but I'm not sure that is a perfect formula.
As I said stupidly, it was great for the first 3 hours, then it caused nervousness that I couldn't figure out how to work through, and it didn't really help with alertness (except at the very first). Then I tried Armodafanil (a close relative) and the side effects were much more severe although my husband thought I wasn't falling asleep as much, so the only reason I didn't keep trying it was because it caused significant stomach upset and I was concerned my Crohn's would start flaring up which I didn't want to risk. But I am very prone to side effects, so these might help others. I was very disappointed.
It would help to know what the appointment was for? A second opinion? An initial evaluation? What specialty is Professor Sheffield working in?
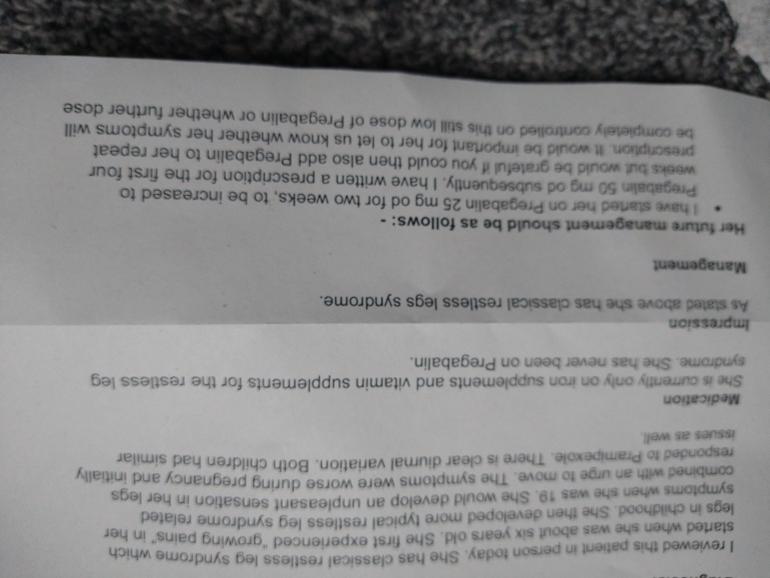
If this is his complete assessment (it’s cut off at top and appears to be a second page) it’s very bare-bones. The first paragraph gives basic history but nothing about severity : how frequent during week, how frequent during the day, what impact does it have on your functioning - sleep disruption, mental health, daytime lethargy, work, school, etc and to what degree. There are no ICSD-3 codes presented. “Classical” Restless Leg Syndrome is not an accepted term (at least in the US) so is meaningless. I think he means idiopathic - of unknown origin - which can be important.
There are no, or few, dosing guides for using Pregabalin with RLS. I do think that the general idea of slowly tapering up on a medication to find the minimum effective dose is a good one. However, these are very low does of Pregabalin. If your PLMD is considered severe (again no guidelines) but - happens regularly (3-4x/wk), begins early in the day (late afternoon, early evening) and symptoms significantly impact your daily functioning - then I’d have expected him to begin with at least 75mg OD and tapering up by 50-75mg more quickly with a max of 1 week between dosage increases. If the PLMD ends up only showing improvement with, say, 300mg 2x/day (Max total daily dosage is 600mg with max single dose of 300mg (drugs.com)), your going to have a long haul to get to a therapeutic dose with a pretty well-tolerated, well known/studied medication. With this slow introduction, it’s likely more costly, the patient suffers longer and the patient may lose patience. Unlike the DAs, there’s little risk even at higher doses of any major side-effects if you’ve tolerated the lower doses well (unless you have other medical conditions that need to be considered).
If you’re suffering now, I’d ask if he can be more aggressive with the increases, as above, with both the daily dosage and time between increases. There’s also an extended release formulation if you have symptoms during the day.
I began at 150mg OD for 5 days, then to 225mg/day, then to 300mg/day. My daytime PLMD had gone away (not necessarily because of the Pregabalin as I was already taking Clonazepam, Gabapentin and Zolpidem). After about 8-12 months, I seemed to lose the benefits from Pregabalin. Like almost all neuroleptic medications, tolerance is part of the deal. I think the “official” RLS treatment guidelines state Pregabalin appears to show benefits for about 6 months. Because of this, I’m working with my doctor to develop a rotational medication regime.
Are you having PLMD when you sleep? How often? Do you have a PLM Index or Arousal Index from a sleep study? Those answers also speak to severity and would be good to show your doctor.
To add to my comment, as Pregabalin does have a tolerance profile that is about 6 months i.e.) you need more to get the same effect, I would want to make the titration as safely and as quickly as possible as all the time you’re tapering up to a thearaputic dose, the clocks ticking on tolerance.
Here is an excerpt from an article by Mark J. Buchfuhrer:
Recommended dosages for treating RRLS/PLMD with Pregabalin
I have taken it for much longer than 6 months with no tolerance effect. I don't know where you got the 6 months, but it is wrong. You can take it for many years before you have to increase it. And the time you are titrating up to the effective dose wouldn't count. I did have to adjust my dose during the first 6-1/2 months - at first 900 mg worked, but eventually I had to increase to 1500 mg. But I haven't had to change it since,
I have never ever been to a sleep study, always wanted to go to one but not sure that they do those in the UK.
Yes, both my kids and myself have PLMD. It starts early evening. I did mention that during the appointment with professor Bandmann. I also mentioned that I was suicidal from lack of sleep at age 28.
One booked appointment is for one illness and he focused RLS. In the UK an appointment is only for one disease. One needs to book another for anything else. Unbelievable!!!
I did mention that I can only sleep alone and kick about all night. I also mentioned twitching toes and restless arms when on Pramipexole.
Professor Bandmann is a specialist for Parkinson and treats RLS as just an annoying thing to have. What a joke!!!
I sometimes only get 4 hours sleep and still function for work every day, which is a blessing!
I have now given up on doctors in the UK. They, do not examine properly and have no time. All they give you is a sick note and standard medication without an examination. I didn't even get a Parkinson check over, even though I mentioned twitching toes! I have to pray to God that prescribed medication works. If not, I don't ever want to grow old with this going on. I am now 55 years old and know already that I will not want to reach retirement age with lack of quality in life.
Rant over. I am sure a lot of guys on here are lots worse off.
Thanks for taking the time to read this.
PS Please excuse grammar...I am originally from Germany English is my 2nd language.
I’m 57 and I also think that, if I knew this was going to be my life for the next 20-30 years, I’d be done. It’s a living hell a lot of the time. I just keep making plans, hoping that the next change will be It.
Same here. Still hoping for a cure and trying to stay in work. Are you still working as well? It's so difficult to keep it up. I hardly travel anymore and going to the movies is out of the question. It's so sad! I am too tired to drive a car as well. It's not safe. Just keep hoping and praying! One day.....there will be help at hand. 🙏
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

") Sorry! Unbelievable that a professor for neurology gets this wrong. Just keep fingers crossed it works at a low dose. Wonder why he did not mention PLMD on report neither!?
Sorry! Unbelievable that a professor for neurology gets this wrong. Just keep fingers crossed it works at a low dose. Wonder why he did not mention PLMD on report neither!?")