Wow! This looks promising!!!! Maybe Vascular ultrasound will surpass the Temporal Artery Biopsy (TAB) as the "gold standard," for diagnosing GCA?
“We think these results implicate that ultrasound should not only be a first-line imaging test in patients presenting with cranial symptoms, but also in patients suspected of GCA presenting with constitutional symptoms, ...If this examination is included in the standard examinations in the fast-track clinics, it may overcome the delay in diagnosis and patients can be treated earlier." ~ Berit Dalsgaard Nielsen, MD,
The problem is that it requires specialist training; not just any ultrasound operator. GCA is still pretty rare so our so called “Centre of Excellence” teaching hospital hasn’t invested in it. It’s cheaper to cut open people’s heads for a reasonable probability of a false negative.
I had the PET scan done which showed up GCA. after loads of tests before hand (did not get biopsy) consultant in hospital asked me if they could use it to try send to America
to put it in place to diognoise GCA in policy’s etc
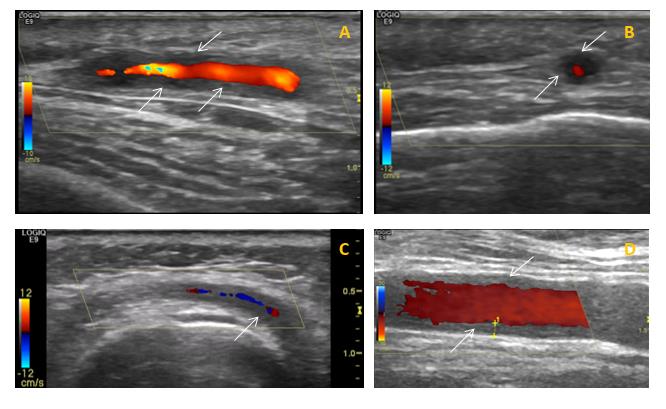
They sent me for one while I was in the hospital, I was watching the screen and asking what they were looking for, "halo's" was the reply. I could see what looked very similar to "A" in the chart you included on the screen but they insisted that they couldn't and dismissed the scan.
Methinks that the operator didn't have the expertise to interrupt the results.
It would be good if they trained more operators in this field.
I thought she might like to read the trial report.
I had the US as the study was taking place in my local hospital and my Consultant was reluctant to stop the pred, although he was sure it had gone into remission. So I had the US as an end test. Halo had gone so he was a happy bunny and I stopped the 3mg pred on 1 Jan and it is the 11th birthday 11 years on 1.1.2019.
Yes that was interesting! Thank you. Explains historically where they came from... as technology advances this method may become more popular! If we can get trained technicians!!!!!!
Doesn't need technology advances - they need trained and experienced technologists and then funding to provide, accommodate and maintain enough devices (what they have are in full use already) and extra staff numbers. That is the most expensive part in fact - the devices are not cheap but it is a one-off purchase and they don't need a separate room. The technologist costs IRO £25K/annumjust for salary, then there are the employer's overheads on top - I'm sure you know that figure better than I do these days, we are 10 years out of date on that, but the total annual cost for 1 technologist must be heading for £50K. Then there are the support staff required.
There has been the intention to role out the u/s diagnosis across the country for some years, it has been known to be as good as TAB since the TABUL study was completed, but there are no facilities to do it. It takes 6 months to complete the training for any sort of u/s and you have to be doing it regularly to keep the skill. Even holiday slows you down and maternity leave almost means re-training.
It's sad - but they can't provide enough nurses to staff the wards...
I've mentioned this before as am living proof it works, we have fast track at Southend and I was diagnosed via Ultra Sound in March 2014, under the care of Prof Dasgupta. I had a negative TAB three days later. He says he prefers US to TABs. Think I'm spoilt here, it was normal for me to have all this technology that I now know isn't widely available.
Scan A reminds me of mine, he showed me as he was doing it and explained the scan. This is what he's been/is striving to roll out in all areas ....The down side is it's a specialised area and not all hospitals have the expertise. I understand it takes up to 6 months to train a rheumie to use US and to be able to interpret the results accurately - then continual use to keep their skills up to date. Prof D is the only one that scans and gives instant results to his patients. His doctors have to have their scans checked by either him or, in his absence, two doctors have to agree the results - double checking all the time.
PS: I had another US in April on my painful shoulders which showed OA - just to confuse matters with the PMR! There were two student doctors being trained by Professor and I could see how difficult it was for them just to get the correct pressure and then to read the scan. I found it amazing to watch.
I think Prof Dasgupta has the Southend running like a finely tuned machine... the rest of the country should take notice! Thanks for sharing your experience T.
This was 2012, since then, progress is slow. Austerity has made a major impact and so have subsequent events.
You can also read about the work of on the net.
EULAR+ARC (European League Against Rheumatism and American College of Rheumatologists) is a committee of PMR & GCA international experts from over 40 countries, if we lost any tiny bit of that committee the progress would be even slower.
EULAR/ARC also has patient representatives from PMR GCA UK, PMR GCA Scotland and PMR&GCA uk North East Support, they have had and continue to have representatives (all volunteers) on many strands related to PMR and GCA. Patient input has been welcomed and respected. Long may it continue.
OMERACT (Outcome Measures in Rheumatology) is an independent initiative of international health professionals interested in outcome measures in rheumatology. Over the last 20 years, OMERACT has served a critical role in the development and validation of clinical and radiographic outcome measures in rheumatoid arthritis, osteoarthritis, psoriatic arthritis, fibromyalgia, and other rheumatic diseases. OMERACT is coordinated by an executive committee and supervised by a steering committee. OMERACT organizes consensus conferences every two years, and employs various other means to stimulate the development of consensus in outcome measurement within the context of musculoskeletal and autoimmune diseases.
Yes, two people who post on this website and patient info are part of that organisation, as well as Patient Representatives.
Last year I was scheduled for a TB, but my doctor changed his mind and ordered the US— which was negative. I’m still suspicious of my diagnosis. My specialist in NYC says GPA can mimic GCA, though rare. I just completed Rituxan (1.5 weeks ago) and am waiting to see if I feel better. The infusions made me feel worse. Those with GCA, are/were your temples tender to the touch? So much so that a bunched up bed pillow would hurt? Because that’s what I’ve been feeling for a couple of years. (Of course, with a menagerie of other things.)
I had a biopsy the day after I was diagnosed with GCA. It was definitely positive, so I was glad to have had it done. However it was very uncomfortable and painful. The surgeon explained that they can anaesthetise the surrounding area, but can't anaesthetise the artery itself as it collapses. For this reason, I think the sooner the ultrasound becomes standard, the better.
Not only that, I had to sign a consent form which stated that there could be a possibility of having a stroke after this procedure. After reading that I nearly chickened out.
Mine turned out positive after taking 60mgs of pred for two weeks. The specimen apparently was squashed. When I had a droopy eye lid I was panicking a bit.
Well I know there are often 'disclaimers for a range of possible 'disasters' relating to tests and ops etc but given the 'unreliability' of the cutting in method I wouldn't do it !! Anyway a clinical diagnosis makes more sense - things like constitutional symptoms seem pretty relevant to me ! Anyway the problem in OZ - or at least where I am in a small regional city - NOBODY here has ultrasound training for GCA - or I suspect even 'heard' about it (as yet).
Good grief, I'm horrified - nobody told me about the possibility of a stroke. Well I can only repeat what I said above - the sooner the ultrasound is available for everybody, the better.
I must admit that I might have signed something without reading it properly. Still there wouldn't be even a remote possibility of a stroke with ultrasound...
No, you're quite right there wouldn't. An ultrascan doesn't need a surgeon surely and there are no health risks whatsoever. No pathology reports and no botch up jobs!
It still annoys me that they missed my halos when they did the scan, why bother doing it if they can't understand the results.
It makes perfect sense to train more people to interpret the results.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.