Hello, I have posted before regarding my daughter who is 10yo but we have just had some very unusual and worrying results which may explain her health issues. She has a long term history of low platelets and I’ve been trying to solve this for her as it has been unexplained. We have strong family history of thyroid disease (she also has DIO1 single/DIO2 double defects) plus a few family members on B12 injections (none have had pernicious anaemia or issues with intrinsic factor discovered though. I am currently going through the motions for B12 investigations as my active B12 is at the bottom of the range).
My daughter has had her low platelets diagnosis since 2016 when she was about 3/4 yo but it could have been from earlier in life. During birth which was very traumatic for her, I had probably been on gas and air (which depletes B12 stores) for near enough 24 hours. During her first year of life she was put on omeprazole (a strong dose) because she could never settle (constant crying) and appeared reflux/allergic.
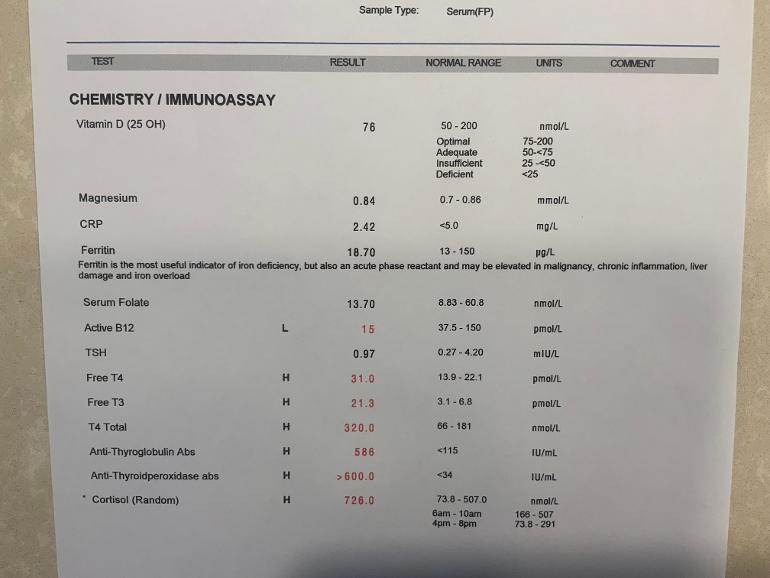
Her results suggest she has an issue digesting/processing certain things as despite eating a very healthy and varied organic diet with lots of meat/fish/eggs, her active B12 is on the floor and her ferritin has been dropping off. She has always taken a multivitamin as well with both these things in. She was only off this for two weeks before this test. The NHS has tested her B12 in the past but this was always total B12 only and this number has always been high in range, I never thought to question it. It is only by chance I tested my thyroid recently with an active B12 test in it and discovered it to be low that I realised hers has never been tested and wondered if she had issues with this as well.
Anyway, it looks like she needs B12 injections to boost her but I’m wondering about whether there is a general digestion issue at play (given low ferritin too) and also what is going on with her thyroid…? The last thyroid test had mildly elevated antibodies but these are through the roof but her FT4/FT3 are ridiculously high also. Cortisol also too high, again! At the time of the test we tried to do a FBC but those bloods didn’t arrive at the lab stable so they couldn’t do them. We know our daughter was suffering from low platelets at the time as she had several large unexplained bruises on her leg (one like a hematoma) and a “cold”.
Anyone with any advice or similar experiences, it will be gratefully received! Thank you!
Written by
RachelP03
To view profiles and participate in discussions please or .
I dont know what to say. . . . . I have 3 grown children and 3 grand children with number 4 on the way and I would not like to be confronted with any of that.. . . . . . Advice I cannot give you. . . . . A hug might be in order. . . . . . . but. . . . . I have always suffered from Dairy problems and if I stay back from dairy my guts are much better. . . . . This may or may not be connected to the inability to absorb B12. . . . . . . It was real bad as a baby.. . . . . not so bad in my 20s but gradually got worse again after that. . . . . .. I think though that if I had continued with consuming dairy my guts would have remained inflamed and my B12 may have gotten worse earlier so I am glad for what I have. . . . . .
Sorry to read. Your daughter needs a repeat FBC. Discuss her blood results with a doctor for referral to paediatric endocrinologist and paediatric dietician.
Hashimoto's thyroiditis can initially cause an overactive thyroid: hopkinsmedicine.org/health/.... That is one possible reason for all the red test results.
Disclaimer: I am a professor of computer science and not a medical doctor. I enjoyed googling health information and that is what I did to try and find something that could explain your test results. It would be good to talk to your doctor about this.
Have her doctors considered the possibility of Functional B12 deficiency?
This is where there is plenty of B12 in the body but it's not getting to where it's needed in the cells so person develops deficiency symptoms.
I'm not medically trained but I would expect doctors to check MMA (methylmalonic Acid) and Homocysteine levels in someone who has low Active B12 (holotranscobalamin).
Search online for "Functional B12 Deficiency" for more info.
I posted a lot of info for adults in this recent thread (may not be relevant to children).
Thank you so much, I will look at all these links. If her low active B12 is due to her history of me having no b12 and breastfeeding her followed by her having a PPI, will getting her levels up be enough so she won’t necessarily be on injections for life or do we think she is likely to need them for life? It’s hard to know cause of course!
"NICE guideline Coeliac disease" says that anyone with unexplained B12, folate or iron deficiencies should be tested. Worth having a look at document if you have time.
If tested in past with a negative result, was the recommended diagnostic process followed?
Coeliac UK page on diagnosis of coeliac disease (mentions children).
A bacterial infection that has been linked to gastritis and B12 deficiency.
Any chance of an internal parasite eg fish tapeworm? There are other human parasites that have been associated with B12 deficiency. I have read of cases where a threadworm (pinworm) infection caused low B12.
One clue that an internal parasite might be present is an increase in eosinophils ( a type of white blood cell). Eosinophil result can be found with Full Blood Count (FBC) results.
Hi, I just wondered two things - did you breast feed her at all and has she been tested for coeliac? Thyroid and B12D go hand in hand and affect each other. You will get to the bottom of it, I am certain. Best wishes
Yes, she was breastfed (I was probably low B12 and iron too at the time). I also had tons of gas and air in her birth (probably almost 24h…!) and then she was on a strong dose PPI for 6 months at the age of 6 months…! All these things I’m sure have caused her issues! We also have genetic defects for thyroid as well so that’s a double hand but low B12 may have triggered the DNA thyroid issues as well!
I'm afraid you would have been very low in active B12 after that and it will have meant your daughter's intake was very poor, even without the PPI. But please get them to check for coeliac and then consider trialling a gluten free diet.
Peripheral neuropathy can be associated with B12 deficiency and sometimes with folate deficiency.
My understanding of BNFC (British National Formulary for Children) is that those with B12 deficiency with neurological involvement should have the following treatment pattern...
A B12 loading injection every other day for as long as symptoms continue to improve (could be weeks even months of them) followed by a maintenance injection every two months.
I can see her folate is not that far above the bottom of range. What has her GP said about this?
Does she have a diet with plenty of folate rich foods eg broccoli, leafy green veg, peas, chickpeas, beans, cereals fortified with folic acid etc?
Might be worth asking her GP if she would benefit from taking a folic acid supplement with the RDA (Recommended Daily Amount) for children. Local pharmacist might also be worth talking to.
B12 deficiency with folate deficiency
It's possible for people to show symptoms even if results are normal range.
In people with both deficiencies, B12 treatment should be started first.
Treating folate deficiency without treating co-existing B12 deficiency may lead to neurological problems.
B12 deficiency can lead to red blood cells that are larger than normal (macrocytosis).
Folate deficiency can lead to red blood cells that are larger than normal (macrocytosis).
Starting folate treatment without starting B12 in someone with both deficiencies may mean red blood cells become normal size but the neurological affects of B12 deficiency continue.
Iron deficiency can lead to red blood cells that are smaller than normal (microcytosis).
In someone who has low iron and low B12 (and/or low folate) their red blood cells may appear to be normal size on Full Blood Count because effects of iron deficiency can mask effects of low B12 (and/or low folate).
I think putting queries about treatment/diagnosis into a short letter makes it harder to ignore an issue. Always keep copies. Paper trail may be useful if there is a need for a formal complaint in future.
Published several years ago so some bits may need updating.
"What You Need to Know About Pernicious Anaemia and B12 Deficiency" by Martyn Hooper
Martyn Hooper is the former chair of PAS (Pernicious Anaemia Society).
"Could it Be B12?: An Epidemic of Misdiagnoses" by Sally Pacholok and JJ. Stuart (USA authors)
Very comprehensive with lots of case studies. There is also a paediatric version of this book "Could It Be B12? Paediatric Edition: What Every Parent Needs to Know".
Please consider seeking support from PAS and B12info.com.
There have been cases of parents being diagnosed with a serious mental health condition when they started treating their child without agreement from child's doctors.
Hi again, just a quick one for both of you, as I was reading something on the PAS site that may be useful - if you are deficient in folate you will not be able to convert B12 to the active forms, and you will lose more B12 in urine than if folate was good. (And bear in mind that folate may be mid range or high in range and you still have a functional deficiency if you can't use it properly - the right form of folate for you can make a difference - but *not* before you've started the B12 treatment). Have a look at the folate section pernicious-anaemia-society....
Seems like it will be both required rhen after any B12 therapy is started! It’s so complex! How do you find out which folic acid suits? Her supplement had the methylfolate form in it! I also read in Dr Chandy’s book that some people find their folate naturally increase as B12 also goes up. A bit chicken and egg really! Thank you for your help though!
Dr Chandy's book is excellent isn't it! I'm no expert, but would think that the patients in question who's folate rose probably were experiencing the folate trap due to inadequate B12. Having the B12 would start the process of availability. And their folate was very low. Dr Chandy says that this effect 'might reduce the need for very high-dose folic acid, so avoiding the known detrimental effects of such high doses'. He doesn't say that it would stop the need altogether, or for everyone. I think the chances of build up of unusable folic are minimised by taking methylfolate, but most people are supposed to be ok with folic. I wasn't, but found by accident that I got a big improvement with methylfolate (having already been taking B12). The genetic (variant/SNP) testing that I did afterwards made me realise why, in conjunction with family history. And I have a problem with MTR (methionine synthase function - connects folate and methionine cycles), so more than one reason why folate availability might get slowed down. That said, I never took a large dose and now only take a maintenance one. Which doesn't mean that your daughter's need is for methylfolate or that she was getting enough of it. Given her low level, I would suspect that something is still not quite right for her, but as her B12 is diabolical, that has to be first priority . Best wishes
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.