Below are some reports and a resulting clinical trial on this exciting possibility. Various studies suggest low cost methotrexate (MTX) can provide benefits to MPN pts, and some authors propose using MTX as a low cost alternative to Rux. If you are not responding or cannot take our current drug options, this seems worth asking your Dr about. Spleen and symptom reductions were a consistent pattern in the reports. I’m considering additional immune suppressants with my Rheum, MTX was not on the list but maybe it will behave well with Rux and even allow a Rux dose reduction.
--
The Reports:
--
“Methotrexate significantly reduces STAT5 phosphorylation in cells expressing JAK2 V617F, … and is comparable to the JAK1/2 inhibitor ruxolitinib”
journals.plos.org/plosone/a...
--
Case reports on 11 MPN pts showed signif improvements in symptom burden. Three pts had beneficial effects on blood counts from MTX.
onlinelibrary.wiley.com/doi...
--
An in-vitro and mouse study:
“suggesting that MTX may potentially be acting directly as a Type 1 kinase inhibitor in vivo (Rux is a type 1 Jak-i) “ …”Strikingly, and consistent with in vitro results, homozygotes treated with MTX have reduced levels of pSTAT5 and pSTAT3”
Spleen size was reduced equal or more than with Rux. (Homozy only, Heterozy mice had no need for reductions, being with low mutation and normal spleens)
--
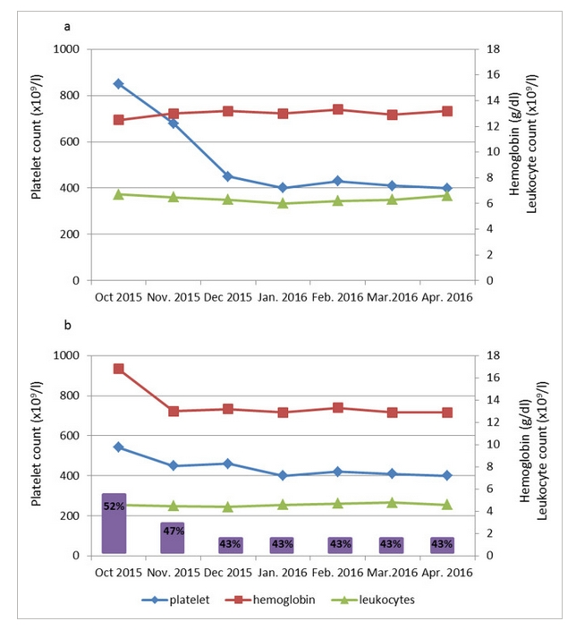
The most compelling case study:
One ET pt was unable to benefit from HU, ANA, or IFN. IFN led to autoimmune in this pt. The 2nd pt was PV Dx, intol to HU and unable to get phlbs. Some of these aspects can be hard to treat pts.
Plots of the effect of MTX here shown here.
The ET pt had rapid normalization of PLT (Blue) The PV pt had same for both PLT and HTC. These plots resemble successful cyto reduction by our usual meds.
They have this misleading statement “Ruxolitinib does not provide significant and rapid reductions of marrow fibrosis and mutation load; analogously, we did not observe significant reduction of the JAK2V617F allele burden over time.”
We know Rux can and does much improve the mutation for many, while it may not be “rapid”. This benefit might carry over to MTX if they measure a long enough duration, it went only 6 months.
“These case reports—being the first on the therapy of MPNs with low-dose methotrexate—has shown in vivo that this approach is efficacious in controlling hematological parameters, systemic symptoms and splenomegaly without inducing additional toxicity”
In context of the “absence of hematological toxicity” the authors say MTX is in league with Rux if a bit lower: “Methotrexate-induced JAK-STAT inhibition was indeed slightly inferior to that observed with Ruxolitinib”
onlinelibrary.wiley.com/doi...
--
Clinical Trial. And finally all these hints of effect have led to a real clinical trial, phase 2 with a respected name, John Mascarenhas, as principle investigator. It tracks everything of interest except the mutation (VAF). The mis-impression of Rux may be why this is missing. It’s 48 weeks on therapy so VAF reductions could happen.
clinicaltrials.gov/study/NC...
--
These reports discuss reduction of inflammation being a possible method of action for MTX. Rux is known to benefit from this action, including a possible reason for its VAF reductions. I understand this is one reason they added Jak 1 to Rux’s targets.
--
If you want info on MTX this is one excellent source from an MD with Sjogrens. MTX is cheap and not high risk in the relevant low dose formats.
sjogrensadvocate.com/medica...
