I've been on Rux since Apr '23. At my recent Dr visit I asked more about Rux. My Dr is experienced with it and has many pts on it. He is an author on some of the early Rux studies. In contrast I was his only Bes pt, which crashed and burned. He has no other pts on any IFN, one quit PEG before starting care with him. So we can assume he has a bias to favor Rux along with that good knowledge.
I asked whether he has any long term PV pts on Rux. He said yes, dating back 10+ years. I asked about any marrow improvements. He said those who hold good blood counts (CHR) tend to show marrow improvements over time. I didn't ask about allele burden (VAF). But in general this idea would track that with IFN, holding CHR with either agent predicts good odds of other aspects improving.
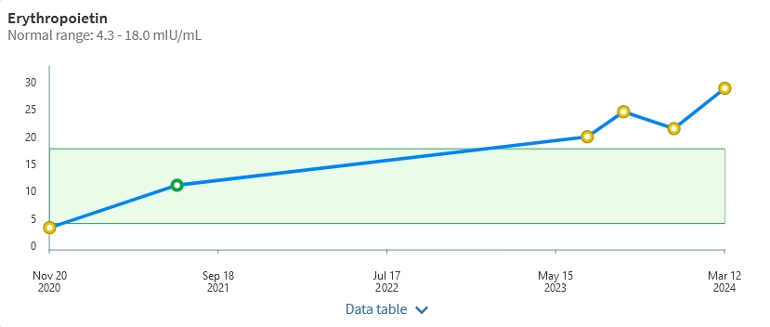
I am holding CHR on Rux as I did on HU and IFN. I noted in a prior post continuing reduction in VAF on Rux. Only weirdness is continuing rise in EPO, well over range now, see plot. I was slightly low at PV Dx as to be expected. I suspect this relates to my Sjogren's, but no obvious link to that either.
Written by
EPguy
To view profiles and participate in discussions please or .
I forgot to note the actual value: 29.1. You're right it's not too far from the 26 reference. My provider tends to have tight refs, for example PLT is 398Max.
Till this latest reading it seemed an outlier, but there is now a trend. We plan to track it regularly while EPO is not normally a regular test.
Possibly if we can fix what ever is doing this I might feel better, a long shot of course. Interestingly 2ndary PV is one listed cause. So is kidney cancer, but a recent UltraSound was clean.
CHR - "complete hematological response" a mouthful for "good blood counts". It's a main result we try to get in our treatments. It implications can be somewhat different in MF where minimum values of PLT and Hb are often a criteria vs max values in ET, PV.
My Dr is in Los Angeles area, I'll PM you since we're supposed to hold some sort of anonymity.
I just saw in your bio that you're holding off the transplant since things are good. In some prior posts there has been discussion that MF "while things are good" is a preferred time to do the transplant according to some MPN experts. In this way the odds of a successful transplant (SCT) are higher. Of course details matter, and the new Jak inhibitors may have changed this idea. But just to be sure you've had that discussion with your Dr.
Glad to hear you are continuing to maintain CHR. I hope that you continue to experience success with the RUX. The increasing EPO is perplexing. Please do let us know what you learn.
It’s very common for platelets to increase temporarily on starting Rux , mine did from 600 to 760 for about 2 months then slowly reduced to now 190, some get bigger increases than I did
Correct, I'm Jak2+ PV. Mutation has been decreasing on both IFN and Rux, now at 5% from 14%. (Like you I've got other issues from A-I -autoimmune- discomforts)
Have you done the full gene sequence to check for other mutations?
I saw in your prior post you had a bad reaction when missing a Rux dose. Is that right? There are some interesting reports on a Rux "holiday". I hope to write about it.
I agree with ainslie, Rux, as with IFN, can take time. But details matter, I see your PLT was at 820 last you reported after a few weeks on Rux.
Yeah missing a dose of Rux left me feeling very bad like withdrawal. I thought it wasn’t worth the pain especially if it wasn’t helping my platelets. Does it work consistently on CALR ? Maybe I should have given it more than two months.
My biggest issue is neuropathy and intense fatigue. My platelets are in the high 500k range on 1000mg HU now. I have rising Myelin Associated Glycoprotein antibodies that attack nerves. I’m about to take IVIG for that but MAG AB usually develops as a result of mgus/myeloma so I’m in a bit of a jam since very few docs know blood and neurology well. Seeing a mgus expert Wednesday to find out if I really have an mgus and/or what I should do. No clear evidence my platelets are causing my problems yet although I’ve read they can cause nerve damage. I had CHR when neuropathy started.
I did have NGS and was told there was nothing bad found.
Maybe relevant to you is "A number of cases have been reported in which a ‘drug holiday’ led to restoration of ruxolitinib response upon rechallenge". And as ainslie says, Rux (like IFN) can take a while for full effect some pts.
This report also notes Calr may be slightly less responsive to Rux, again this is for MF. Also it says some of the newer Jak-is have no reports of withdrawal problems possibly from their longer half lives. I don't think there is any data on these newer ones vs Calr.
You're right about neurology, I consider it a mysterious black art, from having experience to form such opinion. Rheumatology is related and similar.
I also had CHR when IFN blew up, telling us CHR doesn't protect from non blood matters, not surprising. I relate to your fatigue part, it's not at all like "being tired". Sjogren's is full of that.
So good to hear you've found the right medication for you. I hope you continue to do well and all your results are, as you'd like them yo be, very soon.
Thank you for sharing your experience. It always helps to give us confidence, when talking to medical professionals and a better understanding of treatments.
You can see my posts I've been on all three of the common PV meds. All worked great on counts, and mutation went down on IFN and Rux. But a detail with the Bes was a big problem.
On talking to the Drs, we need to assert what our bodies are telling us.
Thanks for sharing. May I ask what tool or software you are using for the plots? Should these be available on my MPN specialist's EHR? I am trying to find a good system to track data and plot visually and if nothing is available, maybe build something in Excel or Google Sheets. Thank you for your response. I enjoy reading your posts, as a data enthusiast and an MPN patient.
The ones that look like this are just screen shots from my provider's portal. Many med groups use My Chart by Epic. Good odds if your provider gives access to your EHR My Chart is hiding somewhere.
This Healthunlocked service is neat that you can paste an image right into the reply. But that doesn't work for original top posts; then it needs to be saved as an image file.
I have some plots that look different for stuff that is not on the portal, like studies or even the Besremi survey I did long ago. I use Solidworks to make these drawings, overkill but doable. Sometimes just MS Paint to modify something, like my plot of 6th year Besremi VAF data.
Excel can make neat plots of data, I've done that for work. But I'm lame with Excel.
Thanks for the insights. I will check with my specialist and see if they can make the data available. I've never used Solidworks and I am vaguely familiar with its use. Believe 3D designers use it quite a bit. Thanks again.
I was diagnosed with PV in 2015 and have been on Rux since Aug 22. My initial dose of 10 mg twice a day caused anemia; I've been taking 10 mg once a day since Nov 22 and my blood counts have been stable (without phlebotomy) since then. Most recent results are WBC 19.14, RBC 4.15, HGB 12.4, HCT 37.8, PLT 408. Differentials show unusually shaped cells; I will bring this up with my MPN specialist when I talk with her in May.
Glad to see that you are in CHR . I think that my MPN specialist at Cleveland Clinic puts as much or more value on CHR as he does in lowering the AB. He has told me not to discount the value of CHR and not to use AB in any decision to switch to besremi when I asked him about switching. He told me he gets about 130 new MPN patients per year over the last 11 years and only has 12 to 15 on interferons, must be a reason for that, I think it is the high rate of complications and side effects on INF's . Sounds like your specialist is not a big fan of INF's either.
After 2 years on HU (as of last summer) my EPO went back to normal from initially low, my Doc said it was because of CHR which I reached about 4 months after starting HU. My AB went from 50 to 19.7 after 2 yr 7 months on HU, I suppose it will start going up again per the Proud PV study. I guess I am lucky so far with the HU . My doc recommends that I stay on HU and not to mess with success by switching to besremi but it is my decision. It seems to me that the longer besremi is available and the more patients taking it, the more complications and side effects I read about so maybe a switch to Jakafi would be a better choice if switching at all. What do you think.
Best to you always and hope that you are feeling better in CHR.
I've had good fortune on CHR from the start, HCT for example here. These years are on HU, Bes, then Rux.
My EPO also went up to normal on HU, it's the recent over range that is mysterious.
I agree with you and your Dr on the significance of CHR. Even if one looks to AB or marrow histology, getting to CHR keeps showing up as an important factor for those 2ndary points.
But one question for your Dr is how many pts in the last two years have selected IFN, vs the 9 years prior? It's only in about the last two years that IFN is widely accepted as normal for MPNs.
--
I've posted on the unexpected ability of HU to improve marrow, you may be experiencing that. Could be worth asking your Dr about it.
Do you have any AB values between the two you noted here? You're right on avg HU goes up after two years, but the Ropeg study I recall did have a small % that held low AB on HU. Have you asked your Dr about experience with AB on HU for other pts?
If you're not having much side effects on HU it does seem good for you and I agree no compelling reason to change. If your AB starts to clearly rise at some point that could affect the thinking. I had the usual fingernail damage and more thinning hair but otherwise ok if the dose was right.
--
IFN vs Rux
In my opinion re Bes vs Rux, based on what we see here, it tracks the studies I believe. Rux has more side effects, but they give plenty of warning and tend to not be life altering. Weight gain seems to be #1, a good thing for me. Increased hair growth is another. Non- malignant skin cancer is the top concern, although I think melanoma has been seen too in a more recent study. Otherwise Rux is a "boring" experience as I joked with Dr this week. In contrast IFN for most pts has a "kick" that lets you know you took it, but otherwise a mostly harmless experience. The catch that your Drs likely refer are cases like mine, and regularly showing up here, autoimmune (A-I) risk. More broadly IFN can do harm unpredictably and permanently; this is unique to this drug among our typical options. One member had sudden onset long term kidney damage. But sneaky A-I's, esp Sjogren's, is a real concern. But to repeat, these "black box" outcomes are much the exception and after ~2 years the odds of them go down (I've posted this somewhere).
If I could re-set time, I'd probably try Bes again, but at an absolute min dose. And I'd skip the flu vax and quit IFN if any neuro symptoms showed at all. I do particularly like the infrequent dosing of IFN. But the boredom of of Rux and its lack of a back box warning for MPN is really nice.
You wrote Rux has more side than Inf effects in your opinion, I think most haems would not agree with that, I discussed adding Peg to my Rux with my expert at Mount Sinai and his view was that Inf can be difficult to tolerate in comparison. Ever thing I read an hear about Rux including my own experience is that there are virtually no side effects in reality for most, some yes but nothing compared to the interferons.
Lots of info to add to the confusion. Keeping PV and MF separate in reviewing Rux is important.
If one excludes anemia, Rux effects do seem low. Top one that near all get is weight gain, even I have solved my weight loss troubles on it. Shingles is a concern. Getting that vax before starting should be a good idea.
This old post has a lot of my pondering worries about IFN. In my case a real premonition. I suspect if IFN were always dosed at an absolute min for CHR (good blood counts) there would be fewer sides and bad outcomes, but still some.
Agree, I forgot to add that Rux PV anemia is not really a side effect, just a proportioned intended effect. Where a trade off can happen is when for example PLT stays high while HCT goes low. I don't know how common that is. This sort of trade off is common with IFN where low WBC limits a dose.
Interesting on Dr V, he's on the board at Ajax therapeutics, working on a 2nd gen Jak-i AJ1-10502 discussed in an old post.
Thank you for the reply and the additional information Also for the additional questions to ask my mpn specialist which I will do at next appointment in July
My first AB was 27% in 2017, about 32% in 2018, 50% in 2021, and 19.7% in December 2023. Started HU in June or July 2021 after the 50% reading that March. I hope to check it again this fall
I think that works out to about 17-18 months on HU at the Dec 2023 reading. That would have it still in the low area (grey line) of the quite familiar plot here. Will be good to see any future readings. As your Dr says VAF need not drive decisions, but does inform.
Hi again, my time on HU from June 2021 to Dec 2023 would be 30 months, I rechecked dates. Yes it will be interesting to see again later this year. I think I have decided to stay on HU until at least Jan 2025 unless something changes in the mean time. Thanks
Your journey is very interesting and certainly complex. So many different approaches to our treatment plans depending on country and doctor, it's great to have the knowledge it helps us make more informed decisions but it also seems to be a minefield despite the research we do. I hope things improve for you, it's been a bit of a journey. Best wishes.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.