A long term study looked at molecular response (MR) vs progression for PV and ET. It was for Rux therapy, although it's possible these molecular correlations apply to IFN too. Of interest is the 12+ year study length and easy to read comparison of MR to progression.
I have a newly acquired interest in Rux so will be sharing my experiences and findings.
--
Some notes:
-One pt with MPL got Complete MR (CMR, undetectable VAF) )on Rux. This is news since I think MPL does not respond well to IFN (comments welcome)
-MR makes a big difference in progression.
-Lower starting VAF (mutation burden) gives better MR.
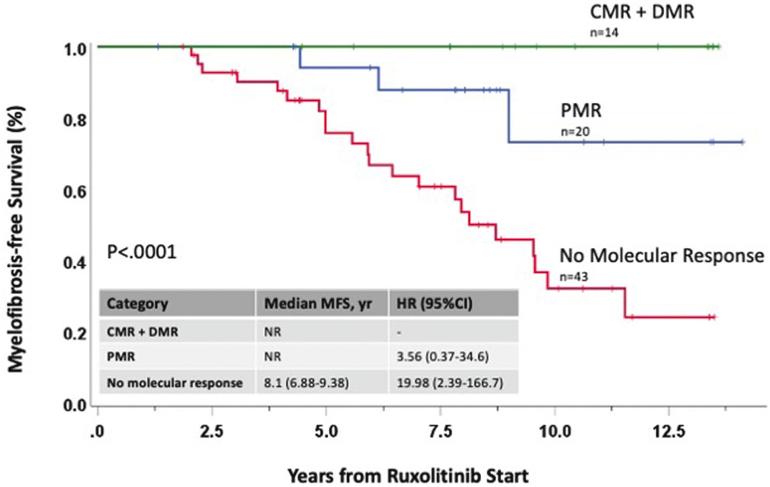
- "All 3 pts who transformed to AML had not obtained any molecular response."
-The plot here is easy to read, green line is all who got to less than 2% VAF. Zero progression over 12 years. This is consistent with 2% limit being important with IFN. Blue got VAF cut by at least half and retains a large progression benefit.
--
- A starting VAF (mutation burden) of less than 60% led to much greater likelihood of MR.
-Compared to pts with decrease to <2% VAF, having no response led to 19X more likely to progress, and partial MR was ~4X more likely.
-Undetectable (CMR) was in 6.5% of pts. This compares well with IFN I believe.
-Tracking MR while on Rux, (or IFN) is a good idea
-It's possible combo IFN+Rux could improve MR for some (my opinion, it's not addressed here)
--
My Dr insists Rux is very good therapy. I'm looking more into why.
good post, Clair Harrison reported similar results for Rux at ASH and I hear the full info will be published soon.
In her trial more it showed 50% reduction in allele in more than 50% of patients ant I think 5 years and showed better than BAT (HU) for event free survival and progression free survival. Pity they didn’t also compare to Peg etc
I have discussed my treatment with Rux with several experts recently and they all mentioned that they have long term patients on Rux for PV doing very well with significant reduction in allele burden.
Curious if these are independent reports, the one above has all Italian names. Seems to be separate since the brief data you show is of a different sort. If there are two separate such reports it does add up well.
Rux has a spotty record in some ways since its early tests were against MF. It's good there but allele reduction and other benefits are a greater challenge. As with IFN, it could point to early intervention as good practice. With the report here, Rux (and maybe IFN) intervention before allele reaches 60% is indicated.
Spotty would be in perceptions, if not actual data, as the discussions below.
Rux's 1st approval and most the data till recently was for MF. In MF many pts have to go off therapy from anemia. So it got a rep as a not durable therapy. (fortunately there is a new Jak-i in the works to address this) And similar to IFN, allele reductions tend to be less than with PV. The report in the top here may be our best clue why, higher VAF gives less response, and MF trends to higher VAF. In PV, many are below the 60% VAF that is relevant here and PV gives more margin to avoid anemia.
So Dr Silver et al may be looking at this MF history and not yet absorbing the recent impressive results with (<60% allele) PV.
Could be PV with >60% VAF is not great for Rux, and best to use IFN, or the combo, since we do see very good reductions there with IFN.
I haven’t seen any data re Rux and 60% VAF and the experts don’t say that and it’s not presented in the CH paper , so really speculation with respect.
I agree Bes may be better in some ways but as I suspect you found out tolerating the drug is the challenge, at about 5-6 years the drop out rate is about 60% according to CH and a recent presentation by Gisslinger, data provided by Hasselbalch, ie the Peg/Bes gurus.
If I could tolerate Peg I would be on it , possibly as a combo
I just saw this reply. The report at top found the 60% cutoff:
"a cutoff level of <60% JAK2V617F VAF at baseline (involving 35 pts, 45.5% of the entire population) was associated with a significantly greater likelihood to obtain CMR+DMR (37.1% vs 2.4%..) as well as PMR (60% vs 38.2%..)."
I assume it was from actual data. But as I noted this will need to be reproduced to take hold.
--
I believe my IFN mess was from the adverse vax reaction. My blood counts, CBC and CMP and more, were near perfect on it even in my worst days. It's possible I would be ok once all settles down. For now I'll see how the Rux goes.
Great to have you back and I am sorry for what you went through. I’ve missed your thoughtful contributions and look forward to the deep dive into Ruxolitinib therapy. Wishing you the best!
I've been a member of MF and PV forums for 7 years and tend to agree with Dr. Silver (see video below ) that Rux monotherapy has relatively little positive impact on the disease course over the long term at least compared to INF monotherapy. Additionally, Dr's. Kiladjian and Hasselbalch have extensive experience with Rux and early MF and have never said they thought it to be comparable to INF in slowing or stopping progression.
However, all three specialists have a highly favorable view about combining INF with RUX in aggressive PV and early MF. Hasselbalch would also like to see the combo tested in early PV.
I find it revealing that the Incyte corp has never made advertising claims about its product (rux ) having major molecular remission inducing capabilities. One would think Incyte would want to advertise Rux as having disease slowing or stopping capabilities comparable to INF if it really did. youtu.be/JHyYQOVy1ec
One important emission you made about what Silver said is that according to YouTube this video was done 10 years ago! A lot has changed since then. By now he will be fully aware of benefits of Rux as all the experts talk to each other, I know Dr Silver has many patients on Rux, ie when he was consulting.
If you want up to date info have a look at vids done by Clair Harrison and Mary McMullen to mention a few, the vids are this year and show Rux for PV and how it lowers AB and increases progression free survival. I spoke to Kiladjian and two other major experts a few months ago and asked if I should try adding Besremi to my Rux, they said no because I had problems with Pegasys, what they did recommend was to stay on Rux because they all had patients on long term Rux doing very well with significant reductions in allele burden
Incyte are promoting the results presented by experts, I’ve seen it and likely more to come.
As recently as 2 years ago Dr. Silver was still saying (see brief video below) "I don't think the [Jak2 inhibitors] are going to change the basic biology of the disease."
Some of the fundamental differences between the hematological and molecular responses PV patients achieve with INF vs RUX may be: 1) the responses with INF may be inherently deeper and more durable; i.e. a subset of PV patients are able to sharply reduce the dose and frequency of dosing or discontinue treatment for periods of 1-5 years before the allele burden and blood counts start rising again. 2) the subset of PV patients that are deep molecular achievers are considered "operationally cured." 3) INF more reliably continues working beyond 5 years. youtu.be/QdEoPlcuf6A
Dr Silver is the world's top proponent of IFN for MPN. This has been to our huge benefit. My 1st Hem said just two+ years ago that IN would not affect my mutation, provably wrong for me. Dr Silver fought these attitudes for 30+ years, we owe him thanks.
But his statement you note conflicts with the latest data and sounds a bit like my 1st Hem. If the study at top here is repeatable, there is a large set of PVs who will greatly benefit from Rux. Reducing allele and stopping progression seems inherently biological to me and for sure beyond just symptoms.
But Dr Silver is right to consider these allele reductions anti intuitive since Rux acts after the mutation rather than on it, but maybe the reduction in inflammation, a known mutagenic, is at work.
If it were true that RUX has a major beneficial impact on the course of PV then why isn't the Incyte Company trying to get it's regulatory status changed from being a second line, behind hydroxyurea, to a first line treatment? Why aren't Incyte's sales and marketing people openly talking about RUX's newly discovered disease progression suppression benefits? Why aren't the Brits and Italians who discovered these benefits publicly advocating for making RUX front line? Lastly, if RUX's newly discovered disease progression suppression benefits are as deep and durable as INF's then it seems to me some of the world's MPN specialists that have years of experience prescribing both drugs would have casually noticed and publicly acknowledged RUX's comparable capabilities years ago.
As ainslie says the data are new. Also these are small early trials phase 2 etc. To make marketing claims I think it requires phase 3 trial which are large and expensive. Esp valid progression data takes a long time. Bes got 1st line only after the large ph 3 in Europe and only via shorter term blood count data.
Rux also is halfway thru its patent term; with 10 years left it will be near expiry by the time a ph 3 is done. Incyte is doing quite well already with Rux, as reported in the business news, it has 3 indications MF, PV, and GVHD so they probably don't need to do much more to keep the $ flowing.
10 years ago, before any phase 3 trials had been done on INF and before any government regulatory approvals for MPN uses were sought and approved, some MPN specialists were, nevertheless, passionately advocating for its use, off label, as a first line therapy because of its obvious disease modification capabilities. We don't see these same specialists (Hasselbalch, Kiladjian, Silver, Gisslinger) passionately embracing the new findings about RUX, even though all 4 of them are experienced prescribing RUX. My guess it's because, based on their years of clinical experience with RUX , they do not consider it in the same league as INF as a disease modifying agent.
I agree the data on PV mod with Rux is new and thin. But a pattern is just starting to show of unexpected benefits. I thought Rux was a dud on molecular etc till I had reason to look into it.
The study at top here needs to be reproduced and the one from Dr Harrison needs to be published. If these events happen, Rux will have a new look that should get attention. But ultimately the combo is the ticket I think.
Naturally we want to see that which ever therapy we're on is effective, I now have a bias to find the good in Rux, to my surprise there is more than expected just popping up.
That said, I way prefer the 1 or 2 /month dosing of Bes, and option to eat grapefruit, and will be trying Bes again eventually.
There is one possible concern with IFN, the post-6 year loss of molecular response for some as I've posted on. Bes guys have hidden this result as I noted. Maybe the combo will help here.
the paper EP posted is 2022, the one Clair Harrison and Co did was only presented to ASH in Dec 22, the full paper fro CH I due out soon. Ie it’s latest info, Dr Silver will know that, as you mention his vid is 2 years ago.
As this info is just out the drug companies and docs have not had much time to promote or consider changing to first line
Agree on the durability of IFN hematological responses. I'm a real life test case I'll post on soon. Rux is known to lose this effect quickly. Less published is the new data on allele response, is this maybe more durable on Rux? And for those with good Rux allele response, does the blood hold up better too?
It seems that ruxo has a minimal impact on the course of MF, but might have a real impact on the course of PV. Indeed, MF and PV are paradoxically both similar and totally different medical entities.
Agree, and maybe the 60% allele cut off is one relevant factor wherein MF has more pts above 60%. Also the anemia margin with PV allows longer therapy.
I think this is so great! I told you in my practice I have been wondering when stuff like this was going to happen. And for me facing two different diseases that require reduction in inflammation/immunosuppression I see the future. And if my MS doc decides he wants to put me on something I would want beta interferon and I think everyone would be interested in that. But JAK inhibitors have so much cross over potential. You are in my prayers and I believe God is taking care of us! Amazing what they are discovering in medicine. I hope this is the answer for you.
Are you going to try Besremi? You noted in another thread. Or hold out for Beta? As in prior posts, the selection of alpha vs beta for MPN was somewhat arbitrary as I recall and beta might have advantages.
I am on Besremi. Have had a total of 5 doses. Really only 3 as the other two were low intro doses. So far so good as far as side effects and numbers are falling. So we decided to stay at 150mcg for now. I found one article that discussed the phenomenon of MPNs and MS and the connection as both respond to interferons. One person in that article was on both alpha and beta. I think you can do that but would have to be watched close. I am going to tell my neurologist I want to give Besremi some time to see as articles from the 90’s shows it works for MS. I am probably one in who knows how many million with both! But trying to just go on and be grateful I have no symptoms of either disease.
« I have run into a few conversations with folks where there is a concern or some hesitancy to utilize ruxolitinib in the polycythemia vera setting due to concern of using their last gun. “Oh, if I utilize this now, then I do not have anything left to use.” A disease that is usually driven solely by that JAK2 mutation and through the JAK-STAT pathway is remarkably responsive to ruxolitinib, and durably so. Some of the reasons we see patients come off ruxolitinib for myelofibrosis after 3 years really do not apply to our patients with polycythemia vera. It is not something that is worth holding off on for a patient who certainly could benefit from it.Srdan Verstovsek, MD: Yes. One aspect of the use of ruxolitinib is that the resistance to it does not develop in a sense that you have additional mutations in the JAK2 gene, like you usually think about BCR-ABL inhibitors, and then there are mutations that prevent imatinib from acting and you need another one. That is not the case here. We have not had anything like this so far, and no testing for it is necessary because it does not happen. It is quite unique, actually, the ability to biologically be active for such a long time without having additional genetic abnormalities leading to the loss of response. I think that is an area, still, of research, and we will see what happens in the next few years.«
Thanks for the good link. The note that additional mutation "does not happen" is a strong one. If it's really that definitive, it could be an advantage over IFN where DNMT3A might arise during therapy. This old post discussed some of that:
JAK2V617F Complete Molecular Remission in Long-Term Follow-up of Patients with Polycythemia Vera and Essential Thrombocythemia Treated with Ruxolitinib
« Until now, complete molecular remission in PV pts has been described only in patients treated with interferon. Our data suggest that a subset of pts who present a rapid and sustained reduction of the JAK2V617F allele burden under ruxolitinib may eventually reach a condition of CMR with prolonged treatment »
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.