Great progress. In the Bes trials they did not find a correlation of dose to VAF drop. But other studies point to higher dosing initially to hit the VAF harder. But at some later point it seems just holding CHR is enough.
My Dr went high as possible for just this reason, but I'm an example of a risk of doing that.
Hi there. My HEM is on the fence on the importance of it dropping as far as disease progression. I won't increase my dose, but will decide before Monday if I reduce it down or stay at 180. I liked not having to get a phlebotomy and having a bit of iron. Maybe a few months at 180 gets my allele down more? Time will tell.
I think with the recent Rux data on VAF vs events, the case is getting strong enough to consider VAF as a criteria. But it's true there is no such data prospectively specific to IFN.
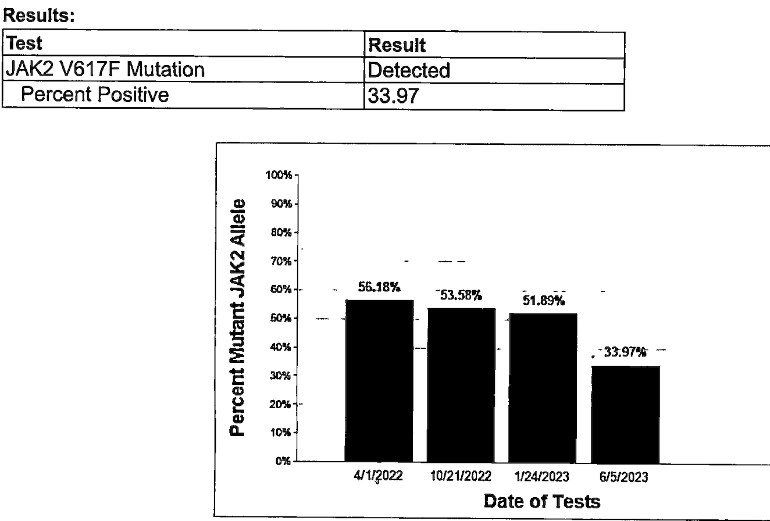
Good news! I do think VAF matters. Less is better.
I also support the notion that we should keep the dose of Besremi or any other medication as low as possible to achieve the primary treatment goal of a complete hematologic response. This reduces the risk of adverse effects. I suspect that over time the data will show that risk/benefit analysis of a lower-dosing strategy is better for the patient. I suspect that the dose needed for CHR will also be a dose that significantly reduces VAF.
PharmaEssentia is rolling out a clinical trail to look at a more aggressive dosing strategy. I expect the data will not support more aggressive dosing as benefiting the patient, but that is the point of doing these studies. Even if more aggressive doing achieves a faster reduction in VAF, I doubt the benefit of a faster reduction will justify the increased risk of adverse effects. We will see what the data shows.
What is tricky is that I most likely would have had to get a phlebotomy if I hadn't increased the dose. Prior dosing, I can usually only go about 4 months before my HCT is over 42 (agreed number as due to my sex). The higher dose kept it down.
lol, yes it is. I was reading about how low iron could cause afib...sometimes you can go down some rabbit holes. Waiting to hear from my HEM on his final thoughts. I'm supposed to inject tonight but might push to tomorrow. He is much more a "slow and study" approach doctor.
good result so quickly, my instincts as per what some others have expressed, maybe wise not to go too fast, you haven’t been on it very long , for some it can a lot longer to get that result and it’s still a good result. Bes probably would have kept lowering it at the lower dose anyway. Worth also bearing in mind that the drop out rate with Peg (according to Gisslinger and Hasselbalch and Clair Harrison ) is something like 60% at 6 years. So it’s a marathon as opposed to a sprint. It’s a good drug but some can have problems, I would be inclined to not rush. Probably wise to discuss with an expert if you can. These are just our opinions as opposed to medical facts, and of course everyone reacts differently somebody else’s experience on here may not be the same for you. Congratulations in the meantime, looks lik it’s going well.
In Dr. Silver's experience (see brief video below) with Pegasys interferon the patient drop out rate due to adverse side effects is 15 - 20%: Dr. Silver advocates using the lowest dose required to achieve a good long term effect on blood counts and slowing of disease progression: youtu.be/TIseFp8NSOY
My wild guess from anecdotal info on the forum is the drop out is some where between the 20% here and 60% you noted re Dr Harrison. Dr Silver's min dose policy may be helping his stats, I might still be in if I'd stayed at 75 of Bes.
My wild guess would be that drop-out rates vary based on the dosing strategy used by the prescriber. Low and slow seems likely to have a lower dropout rate from adverse effects than more aggressive dosing strategies. That is not data, just a bit of applied common sense. We would need the chance to actively compare the dosing strategies between the various sets of data to turn the guess into something more like a fact.
I’ve been trying to decide whether to return to Besremi two months after it caused a dangerous upswing in liver enzymes. My local doc says “do HU” and the Mayo doc I consulted with via zoom yesterday agreed —until I asked if it might be do-able to do Besremi at a low dose. Yes, he said, duration is more important than dose, as long as the interferon gets HCT, platelets and white blood cells in safety zones. I did not ask how long I should wait for that to happen. My liver enzymes are way down after being off the drug, now at the top end of normal, and my HCT is holding strong. Platelets are on the rise, though. I said that Medicare and the clinic are still sparring about the six injections they gave me, but that the clinic indicates (not yet in writing) that I won’t be held responsible for the clinic’s delivery of these injections in a way Medicare rejects. However, going forward, I’ll do the injections myself. Fine with me. I was just following doctor’s suggestions. Dr a la Mayo said “don’t break the bank” to choose Besremi over HU, which is odd, because he was very positive about me choosing it back in December. He seems less keen on the choice now? I know it must be hard for doctors, reading the patient’s tolerances and leanings and guiding or giving in to them, but it is hard for those of us making the choice to be in such an uncertain space medically.
That's an excellent direction to be headed with VAF, congratulations!
Hopefully we'll get more data pointing to the effects of dosing levels on VAF. Would a low dose reduce VAF levels the same as a high dose, just requiring more time to do so? Or does an aggressive initial titration schedule have beneficial long term effects?
The new PharmEssentia dosing schedule that hunter5582 has referred to may give us more answers. Either way, I suspect the reduction of VAF is an important tool in preventing disease progression. Eliminating or minimizing phlebotomy may also offer long term benefits that offset the risk of adverse events from Besremi.
A quick molecular response associated with a low allele burden could mean that the risks of getting secondary mutations is reduced. That’s why a high initial interferon dose could be better than a low dose. The aim is to reduce molecular instability. Genomic instability means more risk of disease progression. So long term low risk of progression could, in some cases, be dictated by a strong initial response to this treatment.
So happy for you!! Im on Besremi too, but have ET. It takes about a year to really kick for many. My thrombos are stable. Just went up to 200 a month ago. I feel so much better now. Keep well. May things get even better!!!!
I’ve been on Besremi (currently 500mcg for 6 months)for a year and a half and my mpn specialist hasn’t checked my Jak2 Alle . I’ll have to ask him next visit . That’s great news for you!! Yayyy!!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.