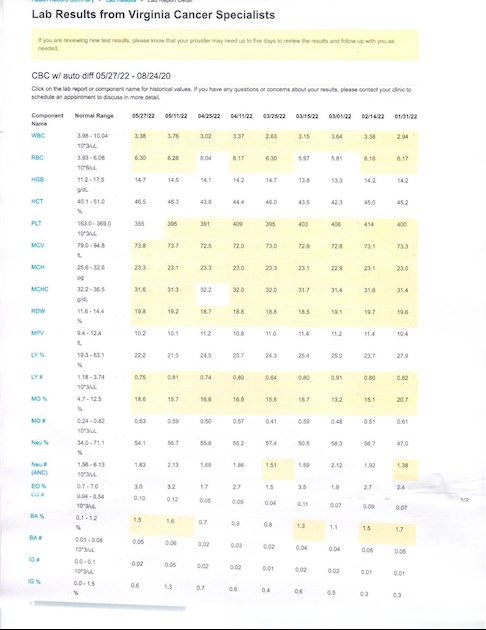
Based on the recent increase in HCT (05/11=46.3%) we decided to up the Besremi dose from 110mcg to 150mcg. First 150mcg dose was 05/25. HCT on 05/27 was 46.5% - too soon for the increased dose to be effective. We are planning to give the higher dose some time to see how it works. If the HCT does not come down, then we will either have to increase the dose again or I will opt for a phlebotomy.
I feel so much better with my iron levels higher that I do not want to opt for the phlebotomy. The concern is that I may not be able to tolerate a higher dose. We do not want the lymphopenia to get any worse nor for the borderline neutropenia to get too severe either. My goal is to control the HCT with medication-only. We will see if that works out. I have also experienced some itching with the Besremi (Pegasys too). Fortunately that has been well controlled with Claritin.
If it appears I will not tolerate the 150mcg dose, the MPN-doc wants me to drop back to 125mcg and try that. He does feel the Besremi adverse effects are dose related. We will just have to see how it goes.
If I do need to do a phlebotomy, I think I will opt for a mini-phlebotomy (250ml) and see how that works. One way or another, we will find a plan that works for me. I am very glad that I have a care team that is flexible and listens. I will be meeting my new MPN Specialist in July. Hopefully she will be equally knowledgeable and collaborative in working on my care team.
I remain hopeful and positive about this course of treatment. We are truly fortunate that our treatment options are improving.
Wishing all of you all the best.
Written by
hunter5582
To view profiles and participate in discussions please or .
The detailed posts that you take the trouble to send in are extremely informative and helpful . They will literally prove to be a guide for another who will walk down this same path . The detailing is exactly what proves to be priceless . Especially considering that not too many are yet on the Besremi path.
I do hope you do well on new dose Thank you for update .I
Warm wishes to you
Hello Hunter what a to do , have to say phlebotomys when needed and prefer them to any increase in my meds appears to work for me,and gives me some sense of some control. I'm sorry l don't have the knowledge you have about treatments or meds,but l know you do and it's a gift we can all share in. Adiewon.
Thank you for all your information Hunter. Do hope your Haemo team along with your own input find the right path for you. I’d be interested in your view on whether Peg Interferon or Besremi are the best treatments for ET as opposed to Hydroxycarbamide which I know did not suit you. I think after 4 years on Hydroxy even though just 500mg daily, I’m getting more side effects . Regards, Fran
Our individual responses to Pegasys/Besremi and hydroxycarbamide vary. As you note, I was not able to tolerate the toxicity of hydroxycarbamide the last time I took it and have responded much better the Pegasys/Besremi. The interferons have been both more effective and easier to tolerate for me. Others have a different experience.
As to which is better in general, it depends on what your goals, risk tolerance, and preferences are. It also depends on understanding how each medication works and which approach you prefer to take.
Hydroxycarbamide is an antimetabolite (cytotoxin). It is a chemotherapy drug that while in common use for MPNs is not FDA approved in the USA for the treatment of MPNs (its use is off-label). Hydroxycarbamide works by interfering with DNA activity in DNA-active cells like hemopoietic stem cells. It is not specific to these cells, affecting other cells in the body too. Because of how it works, hydroxycarbamide can break allele strands and interfere with DNA self-repair. It is a teratogen, mutagen, carcinogen, and appears to increase risk of leukemic progression for people with MPNs. Hydroxycarbamide is a "highly toxic medication with a low therapeutic index." All of that said, hydroxycarbamide is very effective at reducing hematopoiesis and some people are able to tolerate it and benefit.
The PEGylated interferons (Pegasys/Besremi) are immunomodulators. The IFNs bind to interferon receptors, producing antiproliferative effects in the bone marrow. The IFNs are the only medications that appear to be disease altering, reducing the risk of MPN progression and potentially reducing the mutant allele burden. The IFNs can have significant side effects for some, including causing autoimmune issues and psychiatric problems for some who are predisposed. While the IFNs can be effective in the long -term for controlling hematopoiesis, they may take longer to do so. Pegasys is in common use for MPNs, but is not FDA approved for MPNs in the USA (use is off-label). Besremi is FDA approved for PV-only in the USA. Besremi is in clinical trial for ET. The IFNs can e very effective at reducing hematopoiesis and may have greater long-term efficacy, providing the person is able to tolerate it.
As to which approach is better, that is really up to you to decide. If you are finding the adverse effects from hydroxycarbamide intolerable, that is a sufficient reason to switch to one of the IFNs. If you prefer the risk/benefit profile of the IFNs, that is also a sufficient reason to switch. Dr. Harrison gave a nice explanation of how she works with the patient to make this decision in her article "How I treat ET."
So there is not a black-and-white answer to the question of which is better between hydroxycarbamide and the PEGylated Interferons. I feel that the interferons are a better choice for most people with MPNs, but that is based on how I think about MPN treatment goals, risk tolerance, and preferred methods of treatment. Each one of us has to make this evaluation for ourselves. The answer is not the same for everyone. What really matters most is the patient's right to individual choice and having the information needed for fully informed consent to treatment.
Thank you for this link on the treatment approaches of four MPN specialists. It’s very informative and gives me thought on starting IFN therapy to change the course of my illness at its earliest stage. I am curious to know if there is any data on ET/PV patients on IFN therapy who do not develop second cancers or who do develop second cancers despite IFN therapy. For a low risk ET/PV patient, any data indicating a lower incidence of second cancers with IFN therapy may be an added incentive to risk the adverse effects of IFN treatment.
Excellent question! Since interferons have been used for about 40 years in Europe for the treatment of mpn's (I think that is correct), I wonder if there are any retrospective large scale studies that show that interferons reduce secondary cancers, progression, AML transformation, delay progression, and do they improve overall survival. I would think that some researcher would have that data, I have been unable to find it. The short term (5-7 yr) studies such as the Proud PV, Conti PV, Peginvira studies point to a benefit of Interferons over HU or BAT. Best to you.
Thanks hunter, I will read in its entirety. I think I know what to expect from Dr Silver and Dr Hasselbalch. Seems to me that more and more mpn specialists are following their lead. They have been at it for a long time, the kind of data I like to read. Thanks again for this link, I have not seen this article before. Best to you.
Thanks Hunter! This is exactly the type of article I am looking for regarding possible benefits of interferon in decreasing second cancer risks. This article cites past research that indicate interferons may work by restoring normal tumor surveillance since these immune cells are likely impaired in MPN patients. Also of interest to me is the role of statins as an enhancer to interferons. Ever since my MPN diagnosis, my total cholesterol level has been above normal even though my diet and exercise routine have not changed.
Thank you Hunter for the update and hope the increased dosage gets you back on track. I did not know Pegasys was not FDA approved in the United States.
If you have the time, would you give me your interpretation/opinion of Jakafi. I have been on it almost 2 years, and my doctor just keeps increasing my dosage. As you say, the greater the dosage, the greater the side affects. He is only concerned about my HCT and HGB.
I wonder if maybe I should try some different meds - perhaps Besremi since it is available in the U.S.
Thanks for all your time and concern for us in sharing information!!
Besremi and Jakafi are the only two medications FDA approved for PV in the USA. Pegasys is in common use, but it is is used off-label for MPNs. Pegasys is FDA approved for the treatment of hepatitis B.
I think Jakafi is a good drug for some with PV, MF and other MPNs. Whether it is the right drug for you depends on your goals, risk tolerance, and preferences. Jakafi is very effective for specific PV symptoms like pruritis. It is a medication that works very well for some but not for all with PV.
Comparing Besremi and Jakafi is a bit of comparing apples to oranges. The two medications have different mechanisms of action and treat PV in different ways. We each tolerate these medications differently. Besremi (and presumably Pegasys) do have the potential to be disease modifying in reducing risk of MPN progression and allele burden. The IFNs are the only meds that have the potential to be disease modifying in this way.
If you are having trouble tolerating Jakafi, then considering Besremi would certainly make sense. This is certainly something to discuss with a MPN Specialist.
Thank you Hunter for your explanation!! Guess it is impossible to pinpoint, as all drugs work differently on different people. My goal is to live longer and have the best quality of life possible. My Dr. has never discussed the possibility of reducing MPN progression or modifying the disease. His concern is stopping the progression of too many new blood cells, which Jakafi is doing regardless of what side effects the drug causes, Have never had pruritis, thank goodness.
Wish I could get to a MPN Specialist...may be worth a road trip!!
It is totally worth a road trip. to see a MPN Specialist. That is why I have two hematologists. A local hemo-doc who handle on-going care. A MPN Specialist who consults on the care plan. That approach works great.
It is absolutely worth it to see a mpn specialist. In my opinion the longer they have been in practice and able to follow patients throughout their journey with these diseases, the better. Assuming they are a good mpn specialist. Best to you in finding one.
If Rux is not controlling your counts at tolerable doses, that is a good reason to try something different including Bes if Dr agrees.
What side effects (AEs) are your experiencing on Rux? Is it keeping your numbers ok? My Dr has seen good results with his PV patients on it, but I have gone with Bes for now for the deep action it can have as Hunter notes.
Rux is supposed to have advantage over INF by being more specific to the Jak2 problem according to my Dr, but what actually works is what we all care about.
Since raising my dosage of Rux to 15mg alternating with 20mg twice a day, my numbers have improved, but platelets are still 651. I was taking 20 mg twice daily every day. My Hgb is 12.7 and Hct is 37.4, which is good, so the meds are working.
My side affects are fatigue, breathing problems, diarrhea, bloating and abdominal discomfort, bruising badly, high cholesterol, rosacea, and weight gain. I did have blood clots in my lungs from the ET, so I take a blood thinner.
Maybe I am in good shape and I don't know it. Just wish I had more energy to do things!!
I would review treatment options with a MPN Specialist given what you are describing. It can be very hard to sort out what is the different meds and what is the MPN when the symptoms of each overlap. I would be suspicious of AEs from the Jakavi but that is something that needs to be sorted out with your MPN care team. As EPguy suggests, what matters is what works for you - based on your definition of "works." Your goals and preferences are the driving factor in making treatment decisions.
All the bets and wishing you success moving forward.
That is a lot of symptoms. Have most or all of them appeared with starting or increasing Rux? Or as Hunter says, they could be part of your basic MPN, it can be so hard to know. Weight gain does seem very common for members on Rux.
I'm still wondering how Rux could work for me, my Dr recommended it over INF before I selected Besremi. I do plan to continue the Bes for now.
EPguy, yes that is a lot of symptoms!! Probably some are from the MPN and some from the Rux. However, I never had any breathing problems till I got PE's on my lung and that was after I had 5 years of plebotomies and started on the Rux. My blood had become so thick and sticky it wouldn't flow out.
The fatigue and breathing are the most bothersome. The brusing is probably from the blood thinner but no way to avoid that. I am on a statin for the cholesterol and it has come down. The weight not so much but I am doing Pulmonary Rehab twice a week which has help my breathing and hopefully the weight. My breathing has improved so doing some gardening and house cleaning.
Good luck to you in taking the Besremi and hopefully it will work for you like it is for Hunter. Please keep us posted!!
Lymph is cycling between 0.64 and 0.82 recently. Neut has been as low as 1.32 but typically is cycling 1.51 to 2.13. No real change in status since upping Besremi to 150mcg. WIll know more when I do my next CBC on June 13. Not necessarily expecting a big change right away. We will see what happens.
Thank you for the link, Hunter - it is very useful and has made me wish to change Haematologists asap as I am certainly not looked after as well. I hope that you manage to find the correct dosage of your medication to suit you for the next stage of your journey. A heartfelt thank you for all you informative and indepth knowledge and relevant links which you share with us - it really is super helpful.
Hunter - thanks for the update! I have come to accept that finding the best path forward requires a lot of flexibility and trial and error! Each MPN presents differently and our disease is as individual as we are - these facts drive home the importance of a sharing community like we have here (and working with an MPN specialist)! Best of luck on hitting the sweet spot with Bes!
Hope that works out for you. I am in a similar situation in terms of trying to get the correct dose of Besremi to eliminate the need for phlebotomy because I feel so much better now that I have not had one for four months. Besremi at 300 mcg for two doses after initial lower doses brought my hct down to 42 so we lowered dose to 250mcg for next two doses. After that hct was at 46 and dr now wants phlebotomy to bring me below 45. Still trying to figure out dosing. If I get phlebotomy it adds another variable to future dosing questions. Maybe just need more doses at 250 as opposed to higher dose. I really have no idea. All I know is the no phlebotomy thing is a much better quality of life for me in terms of how I feel so trying to find minimum dose for consistent hct control. Sounds like your goal is similar but at lower dose levels. Best of luck.
We do have the same goal in seeking to control the PV without phlebotomy. I also feel a lot better with my iron levels higher. Quality of life is always my primary goal. If you were tolerating the 300mcg dose, I would think about raising the dose back to 300mcg. I expect we will all find that as our iron levels restore, we will need a higher dose of Besremi. This is just basic physiology regarding how our bodies metabolize iron when we have PV.
The other option that I have considered to to do a mini-phlebotomy (250ml instead of 500ml). I would first try a higher dose of Besremi but if I cannot tolerate the higher dose then that is what I would do.
I would note that the HCT can fluctuate up and down on a regular basis. A single read above 45% is not something my MPN-doc is concerned about. I have had it pop up above 45% then be down in the 43% zone with no change in anything I did. We raised my dose when it was clear that HCT was trending up over time. Besremi is not a fast-acting medication. We do have to be patient.
I do understand though why a doc would be concerned when we go over 45%. The protocol is to keep HCT under that number. The doc would feel responsible if someone did have a thrombotic event. Defensive medicine would stipulate to get the HCT down ASAP, regardless of the potential negative impact on quality of life. This is the part where we as patients can assert our right to make our own informed decisions. We can choose to prioritize quality of life over the risk of thrombosis if we wish to do so. I am doing this in the short-term to give the Besremi time to reduce the erythrocytosis. This is my decision and I understand the risk in this approach.
Note that I would not do this in the long-term. If my HCT does not come down soon then I will either increase the dose again or opt for a phlebotomy. Hopefully rusfertide will become another option for us to use in combination with Besremi. Meanwhile, we may have to seek a Goldilocks zone for iron levels if we cannot tolerate a higher dose of Besremi.
Wishing you success with your approach to managing PV.
Great points by you as always. Erring on the side of caution and waiting for phlebotomy as I type this after getting labs showing another small .6 increase in hct to 46.6. Phlebotomy seems inevitable at this point so knocking it out while at md Anderson for labs rather than come back again soon. Will discuss dose increase back to 300 mcg with doc. Thanks and all the best.
That makes good sense. Hopefully a single phlebotomy will take the edge off the HCT without making the iron deficiency symptoms too bad. It is all a balancing act. Do please let us know how you get on.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.