The data were analyzed at 24 months, we know INF needs much longer for its full info to be known. But still interesting.
This trial is a source to compare the main two INFs before Besremi came about. I believe they compared IFNα 2(a) Pegasys and IFNα 2(b) PegIntron. They don't go deep enough here to explain.
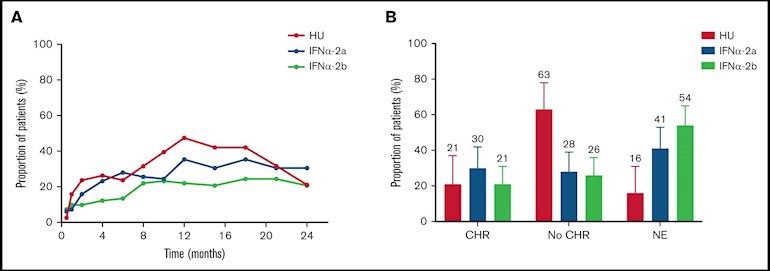
The image here shows CHR for the two INFs and HU. Surprise is the large diff between the two INFs, almost same diff as 2(a) to HU. NE means not evaluated bec of discontinuing.
I've posted before about Bes being IFNα 2 (b). How would it have compared in this study vs the IFNα 2 (a) (PEG) And why did Besremi select the same (b) variant as Intron? They are not telling. It may still come down to the improvements in pegylation, in order of supposed worst to best in this subject it's Intron, PEG, Bes.
Could be the pegylation method matters more than the type of INF.
See reply for one more plot.
Written by
EPguy
To view profiles and participate in discussions please or .
This chart is packed with info. Stand out in their results is DNMT3A mutation (red bar) emerges more often during INF treatment vs HU. This event corresponds to inferior CHR while on INF.
Agree on the peg form, or maybe the type of INF, this data does not address that one. But peg form is plausible and is what we'd all (incl PE as you say) like to hear.
Couldn't open the web pages, got a 403 notice forbidden. Not that I would understand any of it, or be able to help my wife who has MF, as here in Wales we might as well be living in the stone age. We will have a bike ride instead 😊
I checked the link, it's working in my location (USA) But here is the abstract for a start. I agree there's not much us amateurs can do about this info except ask more questions.
--
Abstract
Although somatic mutations influence the pathogenesis, phenotype, and outcome of myeloproliferative neoplasms (MPNs), little is known about their impact on molecular response to cytoreductive treatment. We performed targeted next-generation sequencing (NGS) on 202 pretreatment samples obtained from patients with MPN enrolled in the DALIAH trial (A Study of Low Dose Interferon Alpha Versus Hydroxyurea in Treatment of Chronic Myeloid Neoplasms; #NCT01387763), a randomized controlled phase 3 clinical trial, and 135 samples obtained after 24 months of therapy with recombinant interferon-alpha (IFNα) or hydroxyurea. The primary aim was to evaluate the association between complete clinicohematologic response (CHR) at 24 months and molecular response through sequential assessment of 120 genes using NGS. Among JAK2-mutated patients treated with IFNα, those with CHR had a greater reduction in the JAK2 variant allele frequency (median, 0.29 to 0.07; P < .0001) compared with those not achieving CHR (median, 0.27 to 0.14; P < .0001). In contrast, the CALR variant allele frequency did not significantly decline in those achieving CHR or in those not achieving CHR. Treatment-emergent mutations in DNMT3A were observed more commonly in patients treated with IFNα compared with hydroxyurea (P = .04). Furthermore, treatment-emergent DNMT3A mutations were significantly enriched in IFNα–treated patients not attaining CHR (P = .02). A mutation in TET2, DNMT3A, or ASXL1 was significantly associated with prior stroke (age-adjusted odds ratio, 5.29; 95% confidence interval, 1.59-17.54; P = .007), as was a mutation in TET2 alone (age-adjusted odds ratio, 3.03; 95% confidence interval, 1.03-9.01; P = .044). At 24 months, we found mutation-specific response patterns to IFNα: (1) JAK2- and CALR-mutated MPN exhibited distinct molecular responses; and (2) DNMT3A-mutated clones/subclones emerged on treatment.
Hi EP guy, I don't know if I am reading this correctly or not. I believe that this study says that DNMT3A is the most common secondary mutation to occur during treatment with Interferons. I think it may say that a DNMT3A mutation at baseline leads to more secondary mutations as well as a increase in the DNMT3A AB during treatment with Interferons but not with HU.If I am reading that correctly, what would be the significance for someone with a DNMT3A mutation at baseline (as I have) as it relates to treatment. I am currently on HU, is it better to stay on HU than to switch to Interferon. My MPN specialist says that the more mutations (3 or more) you have the worse the prognosis. I did not see any direct information on prognosis or treatment recommendations with the different mutations, I went thru it fast, maybe I missed it.
I hope to read it more carefully. I've noted before there is no such thing as "I don't have time" only that we select priorities.
I'm not entirely retired yet, so still have a priority to do some "real" work.
It is clear that DNMT3A is more likely to appear as a result of INF than it is on HU. I've seen this connection to INF elsewhere also. I have not yet figured implications for the pre-existing mutation, it's may be in here.
This study looks at many of the mutations we care about, but that's where the time to study it comes in.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.