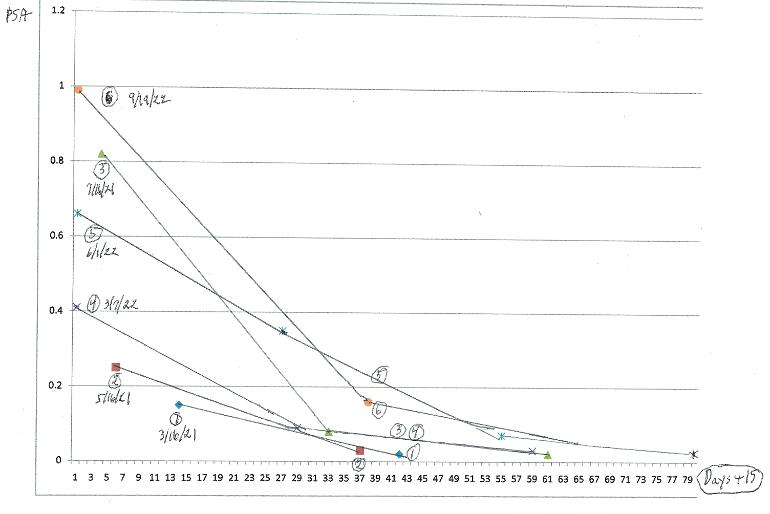
For now I am pausing BAT after six rounds, but would be interested in any thoughts. I am on continuous Eligard, with dutasteride during the last three of the six periods. Each testosterone shot was 400 mg, given at intervals of two months or more. I also take a lot of the usual supplements. Prior to beginning BAT my PSA had been undetectable (<0.02) for some time. The chart shows the evolution of my PSA for each of the six T injections, beginning with day16 after the injection (please forgive my ancient, crumbling chart software and my limited skills with it).
For period 5, the 0.31 value at day 41 (=day 26 on chart) may have been affected by my Eligard shot wearing off just prior to the next Eligard shot since T tested unexpectedly high at that time.
There is a clear pattern of rising curves. It could be that the BAT is putting off castrate resistance even so, but because of this pattern I think it safer, at least for now, to turn my efforts to other strategies.
Written by
cigafred
To view profiles and participate in discussions please or .
I agree with smurtaw. What is the logical problem? (I have been on ADT for about 7 years, so I figure castrate resistance must be getting closer. A Nijmegen Radboud nano-iron MRI (Combidex formerly) showed metastases in the common iliac and para-aorta areas, so action is needed.)
T-cyp. First three rounds done at two-month intervals, next three at three months. I do not use bicalutamide, but on the three-month part my T was low by the end.
cigafred - Thanks for sharing your n=1 data. We all learn a lot from patients like you and smurtaw who openly share your experience in great detail. I also agree that actions that keep the beast at bay and avoid continuous ADT is a better strategy than getting to CR-status and having blown-through most SOC treatment options in 1 1/2 to 2 years.
I'm 9 years out from RALP with mHSPCa and am still managing to cycle short-term ADT and maintain an excellent QOL along the way. Currently doing a dosing experiment with bical. With the boost it gives to T, I am now in the upper 700s and feeling pretty fine without having to do TRT.
Capt'n Mateo - Lots of uncharted territory for all of us advanced patients to navigate, but by sharing our experiences we get more than the stars to guide us. You and the others here are helping to map out those uncharted waters for the rest of us. Sail on, Brother . . . Sail on.
And many Thanks for the way points and better visibility. Ciao - Captain Ahab
You could just be accelerating the time at which it will adapt to the BAT, and the BAT ceases working.
The statistics of attacking adaptive disease agents evidence that it is statistically most effective to hit them with punctuated attacks with everything at once as opposed to the gradual stepped approach that insurance companies used to enforce.
This gives the cancer fewer "at bat" opportunities to adapt.
The clinical trials and emerging standards of care are backing up the mathematical theory.
It's not like voting for a political belief system. Facts are facts.
There is a risk that using BAT early and often helps give the cancer more opportunities to adapt to BAT sooner.
That's why I thought getting a second opinion on this would make sense.
It most certainly was not meant as a personal attack that required a defence.
Got confused. I thought you were the same person/situation.
The logic of what I was proposing remains the same, subject to contrary clinical trials which always overrule logic.
"trying to keep from developing CRPC"
Is there any logic or evidence that BAT works in a way that enables it to prevent CRPC?
There is logic that would support the likelihood that using it early or overusing it is likely to breed prostate cancer cells that are resistant to it's effects.
Why do you think it's early use might plausibly contribute to "trying to keep from developing CRPC"?
I'm just not seeing it. Please explain
(a) the logic, and
(b) why you would not seek multiple second opinions when operating so far away from clinically validated, or semi-validated treatment.
It seems you agree with (b).
I guess the answer to (a) is that it seems to be working well for your bones, though you are doing so many other things (estrogen ADT followed by dutasteride/Casodex) that better explain cause and effect.
How sure are you that you are not operating on confirmation bias.
"My MO and my doctors are adamant that I can NOT change my therapy at this time. "
That's not how responsible docs talk or behave. Especially when operating outside standard of care. No differences of opinion? No heavily layered qualifications?
My recollection is that you are one very very smart and innovative guy.
So I will end where I started. A bit confused. LoL
Have previously posted my own current regimen of long-cycle BAT. I maintain very high Testosterone for 12 weeks with T-cyp every two weeks. It requires very high T to kill PC through double strand DNA breaks and other proposed mechanisms. However, the addition of Dutasteride seems to negate this effect, at least in mouse exograft model.
Perhaps is okay if only used during the low/castrate T cycles but does not appear to be necessary. Personally, I do not measure PSA during High T cycles, only well into my castrate T cycles on Orgovyx. And monitor testosterone then to ensure it is well below 20. As long as the PSA lows are not rising I’m satisfied to continue the program. I’m well aware this is uncharted territory.
Any targets for paired hi/lo DHT-to-T ranges? I also seem to remember that you and others have suggested switching to finasteride at the end of a cycle, since it has a much shorter half-life than dutasteride.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.