Part One, Metformin Anticancer Use - A Review of Current Evidence is here:
healthunlocked.com/fight-pr...
As many PCa patients already know, there is much clinical evidence of metformin being beneficial as an adjuvant to SOC. In fact many patients are currently using metformin, most often via a script written by their PCP. (Sometimes with the approval of their MO, sometimes without.) The original indications that metformin might be helpful were derived by statistical evidence that patients who had been taken metformin (usually for type 2 diabetes) had less incidence of PCa and less-aggressive cancer than those that were not. The following recent research articles look at some of the various potential uses and mechanisms involved in the utilization of metformin as an adjuvant PCa treatment.
1. Metformin combined with quercetin synergistically repressed prostate cancer cells via inhibition of VEGF/PI3K/Akt signaling pathway
Highlights
• Combining of metformin and quercetin synergistically inhibit the viability, migration and invasion of prostate cancer cells.
• Metformin and quercetin synergistically induce apoptosis in a caspase-dependent way in prostate cancer cells.
• Metformin and quercetin synergistically inhibited the VEGF/PI3K/Akt signaling pathway in prostate cancer cells.
Abstract:
sciencedirect.com/science/a...
2. Metformin Use is Associated with Improved Survival for Patients with Advanced Prostate Cancer on Androgen Deprivation Therapy
Conclusions: Metformin use in veterans with prostate cancer who receive androgen deprivation therapy is associated with improved oncologic outcomes. This association should be evaluated in a prospective clinical trial.
Abstract:
pubmed.ncbi.nlm.nih.gov/299...
3. 1948P: Effect of docetaxel-resistance on the reactivity of prostate cancer cells to metformin
Conclusions: These data indicate that reactivity of drug-resistant prostate cancer cells to metformin may depend on the efficiency of metabolic stress-induced EMT. EMT-related metabolic elasticity that apparently increases invasive potential of PC3 cells in the absence of DCX may limit the application of metformin in therapy of drug-resistant prostate tumors.
Abstract:
sciencedirect.com/science/a...
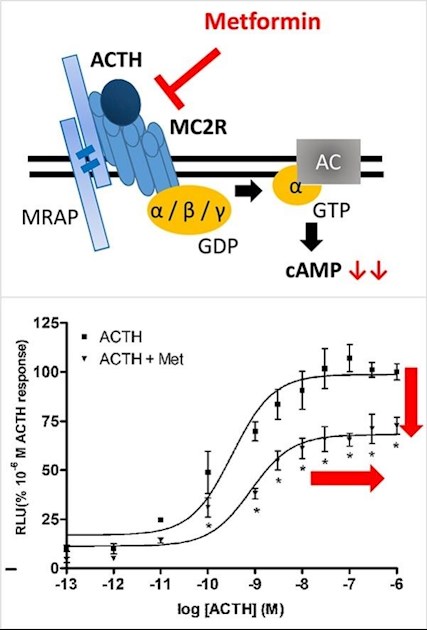
4. Metformin inhibits the activation of melanocortin receptors 2 and 3 in vitro: A possible mechanism for its anti-androgenic and weight balancing effects in vivo? Note: While this research is not specific to PCa, MCR2 & MCR3 are both bad players in PCa. For more info, see here: (pdfs.semanticscholar.org/aa...
Highlights
• Metformin has mild anti-androgenic and weight lowering effects in clinics.
• Melanocortin receptors are involved in signaling systems controlling steroid production and weight.
• MC2R signaling targets androgen production.
• MC3R signaling seems important for regulating weight balance under stressful conditions.
• In a cell model, metformin inhibited ACTH-stimulated activity of MC2R and MC3R specifically.
sciencedirect.com/science/a...
5. Metformin and statins: a possible role in high-risk prostate cancer
Conclusion: Metformin and statins were not associated with BFFS or DFFS improvement in our analysis. However, the small number of patients treated with these drugs limits the reliability of the results and prospective studies are needed.
sciencedirect.com/science/a...
6. Metformin Anticancer mechanisms - Impact of metformin on immunological markers: Implication in its anti-tumor mechanism - Pre-pub proof to appear in Phamacology & Therapeutics, September 2020,
This paper addresses the use of metformin as an adjuvant to immunotherapy. While not currently a major treatment avenue for PCa, that will likely change over time. One interesting note is that the author suggests that metformin use may be contraindicated for immunocompromized individuals.
Abstract
Metformin, an anti-hyperglycemic drug, has been known to have antitumor properties for around 15 years. Although there are a number of reports attributing the antitumor function of metformin to its impact on energy homeostasis and oxygen re-distribution in tumor microenvironment, detailed mechanisms remain largely unknown. In the past several years, there is an increasing number of publications indicating that metformin can affect various immunological components including lymphocytes, macrophages, cytokines and several key immunological molecules in both human and animal studies. These interesting results appear to be in line with emerging data that suggest associations between immune responses and energy homeostasis/oxygen re-distribution, which may explain effective impacts of metformin on immunotherapies against autoimmune diseases as well as cancers. This review article is to analyse and discuss recent development in the above areas with aim to justify metformin as a new adjuvant for immunotherapy against human cancers. We hope that our summary will help to optimize the application of metformin for various types of human cancers.
Link for the Abstract
sciencedirect.com/science/a...
And the full paper via sci-hub:
sci-hub.tw/10.1016/j.pharmt...
Note: Full Papers are accessible via sci-hub.
Stay Safe/ Be Well - K9
PS I do not take metformin, but have been taking it's natural "equivalent", Berberine, for several years.
