On 6 January 2025, the journal BJ Haem published a review article titled Management strategies for patients with chronic lymphocytic leukaemia harbouring complex karyotype written by a team from Padua, Italy. The article summary explains its aims:
"Chronic lymphocytic leukaemia (CLL) is a heterogeneous disease characterised by the uncontrolled proliferation of mature lymphocytes. A subset of CLL patients harbouring complex karyotype (CK) presents with poor prognosis and limited treatment options. This review aims to discuss the current understanding of such patient subset, including its molecular landscape, diagnostic approaches, treatment modalities and emerging therapies. Furthermore, it outlines strategies for personalised management to improve clinical outcomes in this challenging patient population."
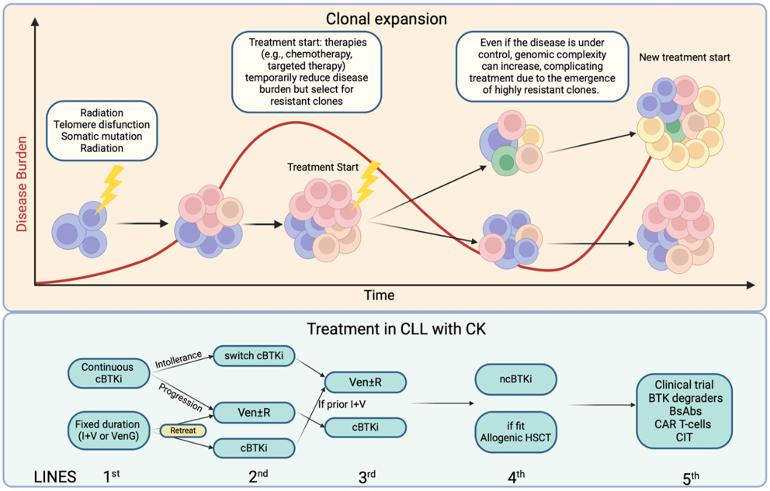
A graphical abstract (see image above) is provided:
"Chronic Lymphocytic Leukaemia patients harbouring complex karyotype presents poor prognosis and limited treatment options due to its intrinsic genomic instability. This review aims to discuss the current understanding of such patient subset, including its molecular landscape, diagnostic approaches, treatment modalities and emerging therapies. Furthermore, it outlines strategies for personalised management to improve clinical outcomes in this challenging patient population."
The review highlights some things we've already known, eg the importance of getting appropriate testing done before each treatment decision. However, it highlights the increasing use of more expansive testing.
" . . . methodologies such as chromosome-banding analysis (CBA), chromosome microarray analysis (CMA) and genome-wide analysis offer a more expansive view of its genomic landscape, which led to the identification of chromosomal abnormalities in a relevant number of patients with CLL, being either quantitative, as for instance monosomies or trisomies, or qualitative, such as translocations, deletions, insertions and isochromosomes.² Of note, complex karyotype (CK), classically defined by the presence of at least three chromosomal alterations in the neoplastic clone, can be found in 15%–20% of patients at diagnosis, but such percentage goes up to 30%–40% among relapsed/refractory (R/R) cases.³, ⁴ In addition, up to 5% of patients with monoclonal B-cell lymphocytosis (MBL) can present with a CK in their clone.³"
It also highlights some things we might not have appreciated: that carrying five or more chromosomal abnormalities has a deeper impact on disease course than carrying fewer abnormalities (eg the previously defined three abnormalities).
"Although karyotype analysis through CBA has been widely used in haematology to refine diagnosis and prognostic stratification of several haematological malignancies, it has been widely accepted as prognostic and/or predictive factor for CLL only in the last few years. Currently, CBA is recommended to be performed before starting treatment by NCCN and the GCLLSG guidelines.⁷⁰, ⁷¹
While in both guidelines CK is defined by the presence of three or more chromosomal alterations, recently accumulating evidence points out the fact that CLL carrying five or more chromosomal abnormalities has a deeper impact on survival and response to novel therapies. Targeted therapies, such as second-generation BTK inhibitors or venetoclax-based combinations, can overcome the negative impact carried by a less-complex karyotype (i.e. <5 abnormalities)." (my emphasis)
There's a lot more information in the full paper which you can read here:
Serafin A, Ruocco V, Cellini A, Angotzi F, Bonaldi L, Trentin L, et al. Management strategies for patients with chronic lymphocytic leukaemia harbouring complex karyotype. Br J Haematol. 2025; 00: 1–10. doi.org/10.1111/bjh.19986
CLLerinOz
Note this is an unlocked post so anyone even those outside our community can read it. If you want to ask a question related to your own situation, it's advisable to start your own locked post. There's more information about locked and unlocked posts here: healthunlocked.com/cllsuppo...
